

Purpose
The aim of this study was to explain the patient assessment experiences of the medical staff responsible for customer satisfaction and quality improvement at their respective medical institutions.
Methods
This was a qualitative study using a focus group with quality improvement or custom service department managers. Participants were selected using purposive sampling. Data collection was conducted with seventeen participants divided into three focus group interviews from July 3 to 5, 2017. Each interview took an average of 1 hour and 40 minutes. Transcribed data were analyzed using qualitative thematic analysis.
Results
Base on the analysis, four categories and eight themes were derived. The categories were: 1) what is the quality of hospital service? 2) between directionality and timeliness, 3) variations in recognition and application, and 4) changing in hospital culture Conclusion: The assessment of patient's experience has spread a patient-centered culture and elicited significant changes in the behavior of medical and hospital staff. However, the survey instruments and procedures for assessing patient experiences need to be continuously improved, and additional research is required to secure evidence related to patient experiences.
The aim of this study was to explain the patient assessment experiences of the medical staff responsible for customer satisfaction and quality improvement at their respective medical institutions.
This was a qualitative study using a focus group with quality improvement or custom service department managers. Participants were selected using purposive sampling. Data collection was conducted with seventeen participants divided into three focus group interviews from July 3 to 5, 2017. Each interview took an average of 1 hour and 40 minutes. Transcribed data were analyzed using qualitative thematic analysis.
Base on the analysis, four categories and eight themes were derived. The categories were: 1) what is the quality of hospital service? 2) between directionality and timeliness, 3) variations in recognition and application, and 4) changing in hospital culture.
The assessment of patient's experience has spread a patient-centered culture and elicited significant changes in the behavior of medical and hospital staff. However, the survey instruments and procedures for assessing patient experiences need to be continuously improved, and additional research is required to secure evidence related to patient experiences.
Patient-centred healthcare starts from a changed perspective [1, 2], which is to break away from traditional illness-oriented healthcare and to understand the patient as an individual with unique value. Patient-centred is generally defined as 'respecting the desires, needs, and preferences of patients in the decision-making process by building partnerships between care providers, patients, and patients' families and ensuring education and support that patients need to make decisions and participate in their own care' [3]. Patient-centred medication (regardless of whether or not it achieves the goals it aims to achieve, such as improving the quality of health care and improving health levels) itself is considered essentially the right thing to do. Patient-centred is considered to be a key component of quality of health care and an essential component of health care system performance assessment.
A patient experience assessment (PEA) is a survey that evaluates the degree of patient-centred care at a medical site, such as a patient satisfaction survey. In many countries, customer satisfaction surveys have been conducted to assess patient-centred healthcare. In January 2017, the Health Insurance Review & Assessment Service (HIRA) in Korea started a trial implementation of the assessment service and systems [4]. In July of the same year, the first PEA was conducted in earnest. The first PEA conducted by the HIRA was for patients who were discharged from the general hospital [5]. The questionnaire consisted of 24 questions in six areas, including nursing and medical practices, medication and treatment processes, the hospital environment, and patient rights. The survey was conducted by telephone. The assessment results correct the distribution in consideration of different patient configurations by hospital and yield comparable patient experience scores by hospital [6]. Therefore, the PEA, which identifies experiences during hospitalization, is reported to be more descriptive of differences in practice by hospital than the patient satisfaction survey, which examines the patient's expectation and satisfaction [7].
It is reported that positive patient experience is related to increased hospital profitability [8], which directly affects hospitals and shows higher nursing service satisfaction and hospital reuse than patients who receive Customer Experience Management (CEM) [9]. In the future, hospitals will be paid medical quality support costs from the government based on the results of the evaluation. Therefore, hospitals are making various efforts to provide patients' experiences more positively.
The experiences of healthcare providers during the early days of shifting from disease-centred to patient-centred healthcare have important implications for the Korean medical community. The PEA will induce a change in the medical culture [9], and it will be necessary to look at the experience of the process as well as its consequences [10]. Quality improvement (QI) specialist is a mainstream nurse dedicated to quality management in hospitals, who proposes a service delivery system to efficiently provide interdependent medical field work, and plays a role in communication for cross-professional cooperation and coordination [11]. A holistic understanding of QI specialist's experience in patient experience surveys is thought to contribute to the development of the theory of cooperation and coordination in nursing practice.
The FGI study has advantages [12], such as, it helps attain an understanding about complicated PEA situations and identify major theme or variables affecting PEA in the hospitals. This study attempted to explore and to provide an explanation for the experiences of the quality improvement activities regarding PEA. These efforts will demonstrate the difference between patient satisfaction surveys and patient experience surveys in the practice of the medical field, and how changes are occurring in the attitudes and perceptions of health professionals after applying the PEA that were observed. This study will provide an opportunity to discuss the direction for a more valuable PEA.
This qualitative study used focus groups to explore the experience of quality improvement (QI) specialists who have experience applying PEA (PEA) to hospitals.
Participants were selected using purposive sampling by e-mail among the members of the QI Society. E-mails were sent to members in charge of quality management working in hospitals that received a trial evaluation of patient experience medical institutions, and seventeen of them agreed to participate.
Data collection was conducted through three focus group interviews from 3 to 5 July 2017. Interviews ranged from one hour to two hours and ten minutes. The focus group consisted of 7 to 10 participants with rich experiences related to the application of the research theme [13], that is, PEA. The focus interview was conducted with semi-structured questions. The first question started with'Please tell me about your patient experience evaluation preparation and evaluation process experience'. Focus group interviews were conducted with 2~3 researchers participating, and we served as interviewers and field observers. Immediately after the interview, we performed an initial analysis with the interview contents and field notes.
Transcribed data were analysed using six-stage qualitative thematic analysis by Braun and Clark [14]. All interviews were transcribed by a trained research assistant. Analysis was performed concurrently with data collection. We re-read the data to familiarize ourselves with it. Thereafter, we generated the codes, which were pithy labels achieved through capturing both a thematic and conceptual reading of the data in the transcripts. To search for themes, we compared the similarities and differences in the code and categorized them into similar semantic units. We reviewed the themes in relation to the entire extracted dataset, created a detailed analysis, identified the essence of each theme, defined and named the themes for further discussion of themes. Finally, we wrote an analytic narrative and contextualized it.
The analysis process was carried out manually by our research team. We shared and discussed our experiences and opinions regarding data collection and analysis via email. Three researchers possess prior knowledge of QI activity in hospital, and two researchers are experts in conducting qualitative research.
Prior to conducting the research, this study passed the research ethics review of the university (HYCU-IRB-2017-001-1) with which the researcher is affiliated to ensure the human rights of participants. We obtained written consent from the participants, after explaining the purpose and procedure of the study. They were also informed that the data would be used for research purposes only and the recordings and manuscripts would be kept on a single locked computer.
For ensuring rigor in this study, we applied the criteria proposed by Sandelowski [15]; reliability, fittingness, auditability, confirmability. The data of this study reveals the actual experiences of the QI specialist. The FGI were recorded and transcribed verbatim. We tried to ensure the accuracy of the transcriptions by comparing the recordings with the transcriptions. We also identified the adequacy of citations to support themes derived from the data. The participants' narratives were described and interpreted based on the derived themes. We read the manuscript multiples times and clearly described the analytical procedures for deriving initial codes, sub-themes, and themes. We also tried to maintain neutrality throughout the research process.
The participants in this study were those who were directly involved in the PEA at the hospital where they worked, and all but two were nurses. All participants had at least three years of QI-related work experience (Table 1).
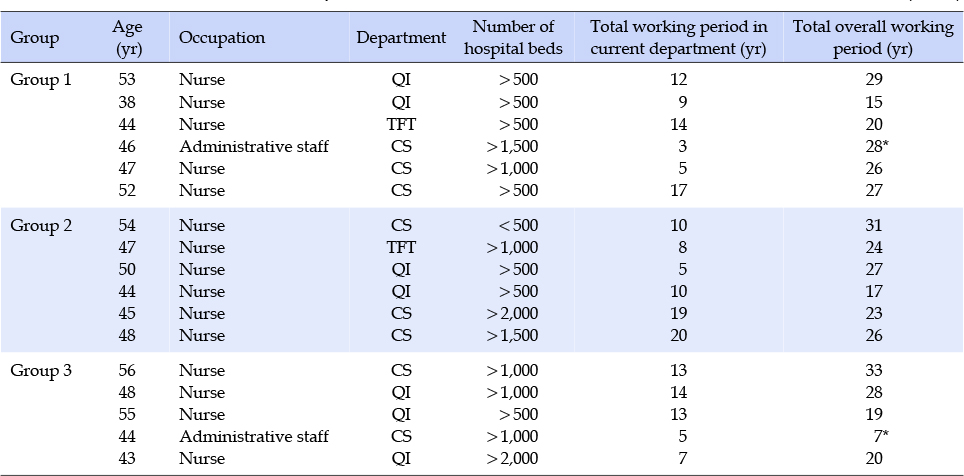
Table 1
General Characteristics of Participants (N=17)
After analysing the focus group interviews, the four themes and eight sub-themes were derived. Four themes are: 1) what is the quality of hospital service? 2) between directionality and timeliness, 3) variations in recognition and application, and 4) changing in hospital culture (Table 2). These themes were illustrated the QI specialists' experiences to implement of 'patient's experience' in hospital.
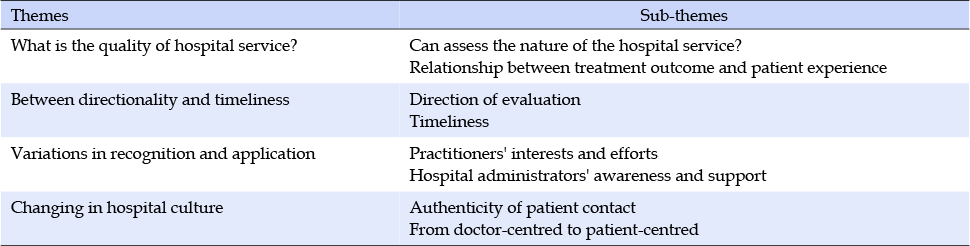
Table 2
Themes of Experiences for Application of Patients Experience Evaluation in Hospital Assessment
This theme was a major concern for participants as they prepared and conducted multiple hospital service assessments as heads of quality management departments. Their concern about myth for quality of a hospital, it was including not only the result of the treatment of a disease, but also about the tenderness and kindness associated with healthcare. This included concerns about how the treatment, care, and nursing of patients were reflected in the quantitative assessment and whether society's requirements of healthcare delivery were fulfilled.
Quality of medical service should be supported by the quality of care, because the results from the patients are not all good when they are discharged. As I have experienced, is it probably the result of the final feeling that the patient or family has in our hospital, the feeling of communicating with the staff in the hospital or the facility or is it a feeling for the entire hospital?.. I thought it might be the last feeling left in my head which becomes the last experience that determines the quality I feel in the hospital. - FGI 3
This was drawn from the participants' concerns about the influence of patient outcomes and stories about the hospital assessment. Many concerns were expressed that the patient's experience during hospitalisation could depend on the outcome of the disease. The patient's treatment outcome is the most influential factor on the assessment rather than the level of the hospital.
From a patient's point of view, good treatment prognosis might be quality? If looking at it from the patient's position, with good operation, and when I came up with what I expected, it didn't matter whether I was waiting or the issue of doctors. Just when I became a patient, when treated for it and then it feels better and then you feel something like everything is happy? - FGI 1
This was a question that the participants in charge have constantly asked themselves while undergoing numerous hospital assessments, and reflects their concerns. Participants said that there is a need to reflect on considerations regarding the inherent function and nature of the hospital and the culture of excessive assessment in our society.
Because the quality of medical care that patients feel is to perceive the nature of our hospital as quality in a distorted way, the hospital assessment or say, the CS satisfaction survey, I thought these were the biggest rats for us. - FGI 3
Participants who were involved in institutional assessments or demonstrations of processes that need to be followed prior to the implementation of the PEA agreed to move to the patient-centred approach. However, some participants raised questions about not considering the Korean culture, not giving adequate time to the hospitals so that they could be prepared, and about the validity of some of the published assessment items. Most participants said that they should begin to change the hospital culture to become patient-centred and to accept that this is the beginning of change.
It's the right that inserting the experience of a patient's position into the quality of medical institutions fits the trend of the times, but let's do a little bit of assessment now and connect with it later. As a result, assessments are more urgent than hospitals worrying about real concerns and the patient's treatment quality. I don't think the patients want it. I don't think I'm going to forget about the essence of it in this day and age. - FGI 1
This theme was derived from the participants who applied for the PEA at each hospital from the time they were ready to apply, agreeing to changes in the assessment where a patient-centred emphasis was placed. Although implementation was prematurely started, most participants agreed with the change that emphasised a patientcentred focus.
The survey itself is actually turning into a survey that can change the doctors, nurses, or behaviors we provide, compared to my previous satisfaction. ... In order to get better results, we have to move the doctors and move the nurses, and then something changes even if it changes into something better. In the process, I think then it is possible to head towards an assessment that could change some people: the hospital's medical staff. - FGI 2
This theme emerged from most participants arguing that public relations should be considered prior to applying the PEA. Patients whom the participants met while applying the PEA had difficulty in separately evaluating their treatment outcomes from the hospital experience and lacked much understanding of the difference between medical service satisfaction and assessment. Nevertheless, all participants agreed that it is an appropriate time to change the PEA.
I hope there is something commercially available in our country, and I think this is a little better than the existing satisfaction survey. Didn't we make this come in too soon when you introduced this? I think [so]. - FGI 2
This theme was derived from the fact that the perception of patients' experience assessments varies. The application varies depending on the degree of support for the hospital's interest and quality management, as well as the level of awareness and concern about the hospital's assessment.
There were differences in the size and tasks of the quality management departments of hospitals. In addition, the understanding and support provided by the management and medical directors differed among hospitals. There were some participants who were already preparing for the PEA, while others responded to it prior to the change in the QI system in the hospital.
Is there any variation in each hospital and various conditions are different? Wouldn't it be dangerous to just disclose the discrimination by reflecting it as one condition? So I think it's a result of giving up on a hospital that what I feel during the assessment is that the results will be something to give up on a hospital that can't work well and to give support to a few hospitals that are doing well. - FGI 3
All the participants had been in charge of quality management for many years. Some participants were overwhelmed by the task of responding to hospital assessments from several institutions each year, while others were still preparing for a new round of assessments.
Our quality management is [about] what's going on, such as electrical wiring behind the fluorescent lights, how efficient and safe it is, and I'm very interested in this. But the patients here are interested in whether it's a fluorescent lamp or a chandelier. - FGI 2
The level of awareness of the hospital management executives was also important in the application of PEA. The perception of management executives was that the PEA was a new version of a consumer satisfaction assessment and it was accepted as an obligation or formal convention. However, many participants said that the active support of management had the greatest impact on the outcome of the application of PEA.
This theme was derived from the fact that all participants who applied the PEA to each hospital expressed that the culture of hospitals was changing to patient-centred, through the application process and subsequent results. Several hospitals have already improved many aspects of their hospital's culture, but it was noted that changes are emerging at the point of contact with the physician closest to the nature of the medical service. This is not just a matter of service but also of authenticity; the medical staff is constantly engaged in modifying the space for the patient, and provide nursing care for the patient during the patient's stay at the hospital. The participants were told that the changes in physicians were particularly noticeable, especially when providing the PEA on the phone.
Experience assessment seems to have made a greater progress in care than in satisfaction. It seems to have been research that changed the culture. It was a meaningful first hospital assessment but there was a limit to [the] changing of staff attitudes inside the hospital, and in that aspect, experiences seem to come and so we look at the patient experience or satisfaction from a new perspective. - FGI 3
Minor but important changes were made at the point of contact with the patient, such as making eye contact, providing explanations slowly, and clarifying the patient's questions. This change has been communicated sincerely to the patients by the hospital staff. In particular, the change in doctors was a great change for the patients.
Until this change, quality managers had made a long-standing effort to improve the quality of their hospital culture. It resulted in an opportunity to recognise the sincerity of the doctors towards the patients.
Participants said that the biggest change experienced in applying the PEA was to move the focus of the hospital from doctors to patients. This paradigm shift at the centre of hospital culture is natural, and it is this part that must be accepted and changed in the medical culture in Korea. They seemed to be proud that the beginning of the hospital's transition from the doctor to the patient was reflective of what was happening in the field.
As we get this pre-assessment now, all we have to do is throw away the idea of looking at the patient [as] we used to, and put them in our chest and heart as a person that should be respected. I think doctors are facing this challenge ... I think it's this assessment that makes them challenge that. - FGI 2
The results drawn from this study encompassed three areas. First, QI specialists in charge of PEA recognised patient-centredness as a critical area in medical institutions via this PEA. Second, they pointed out that the current evaluation system does not properly evaluate on-site experience due to the limitation of experience evaluation tools, and future improvement is necessary. Third, the PEA included objective statements about providing medical services and specific information on QI compared to the patient satisfaction survey; however, subjective factors could not be complete eliminated.
The patient experience is a representative quality assessment area viewed as patient-centred [16]. The US Institute of Medicine proposes a patient-centred service with safety, effectiveness, timeliness, efficiency, and equity as a requirement for healthcare. [3] In the healthcare service assessment, the patient-centred approach has long been the subject of patient satisfaction surveys, and recently the patient's experience of assessment has become a major area of hospital services [17, 18]. Previous studies have indicated that in various assessments, medical institutions still lacked a response to the needs of patients [7, 19, 20]. A patient-centred approach is difficult to provide in the medical field. Medical care service is such an area where the biggest change is expected through the PEA.
Healthcare service assessment and accreditation systems were implemented to ensure that hospitals would provide high-quality medical services [21, 22], and healthcare staff have acknowledged that accreditation has had a positive effect on QI [22, 23, 24]. Although the patient-centred approach is at the centre of this accreditation, there is concern that a fair assessment may be difficult because patient-centredness cannot be independent of the effects of patient preferences and the underlying diseases. When the patient experience becomes a major focus of hospital assessment, the emphasis shifts to the consequent patient experience questions, rather than the veridicality of the patient experience [25].
The subjectivity of satisfaction cannot be completely overcome by objective experiences, and the fairness of the assessment cannot be ensured. The quality of healthcare is defined by the times and existing institutions. In particular, the quality of patient experiences and the path through which such experiences are gained must be shared by all members of the healthcare system. Unlike satisfaction, which is the outcome indicator, experience includes the context of process indicators, such as the patient's experience with service performance and frequency, and it is more objective [17].
Assessment is also important for the precision and validity of the tool, but acceptance depends on the procedure and method used. Since the purpose of evaluating patient experience was to evaluate services between hospitals, much confusion arose due to improper corrections in areas that are difficult to evaluate, or where the evaluation score is significantly lower, such as in the doctor's section [21]. It is necessary to reflect on whether the current tools for the PEA are adequately included [26].
To overcome the limitations of the PEA in previous satisfaction surveys must be improved. First, there are concerns about the validity of the items in the PEA. Priority should be given to what the patients want in healthcare rather than the ease of assessment. Institutions with good outcomes in PEA should be able to clearly interpret why the patient experience. Above all, patients' experiences should be measured objectively, then the results should be disclosed and utilised for improving hospital services. To enhance the objectivity and utilisation of patient experience evaluation, related research should continue.
Lastly, to improve the quality of medical care, we need to evaluate people's experiences using medical institutions, promote the need for public participation, and educate them on the evaluation process, survey contents, and utilisation of results. In expanding the scope of national health insurance coverage, the public should be properly educated about the use of healthcare services and participate in its assessment to recognise the obligations and rights as Korean citizens.
The system of PEA may vary depending on the country, time, the socio-cultural background. As an early evaluation, this study has limitations in tools, evaluation procedures, and sharing results in South Korea. Based on continuous research and clinical application experience, development of an evaluation system that can appropriately evaluate field experience, including evaluation tools, is expected in the future.
As a result of interviewing the hospital quality managers, the PEA confirmed that the patient-centred culture was expanding, and the behaviour of the hospital staff was changing. However, in order to have a positive impact on the quality improvement of medical care in Korea, the acceptance of PEA and the utilization of results needs to be improved, ensuring the validity of patient assessment items and continuous improvement of assessment methods and the procedures.
This research was supported by the Korean Society on Patient Safety & Quality Improvement Nurses (KoSQIN).