1Department of Nursing, Asan Medical Center, Korea.
2Department of New Health Technology Assessment, National Evidence-based Healthcare Collaborating Agency, Korea.
Copyright © 2015 Korean Academy of Nursing Administration
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
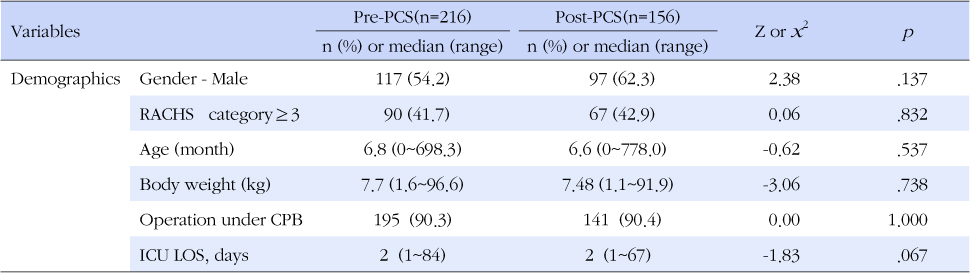
PCS=Practical communication strategies, RACHS=Risk adjustment classification for congenital heart surgery method, CPB=Cardiopulmonary bypass, ICU=intensive care unit, LOS=Length of stay.
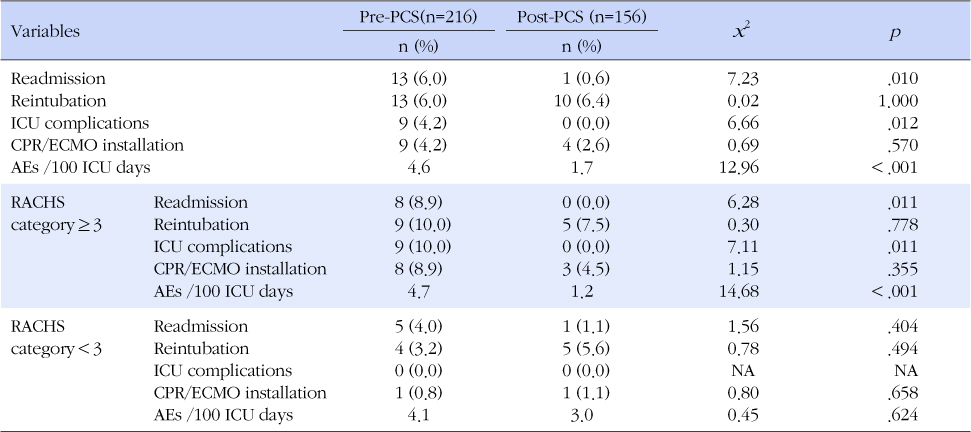
PCS=Practical communication strategies; RACHS=Risk adjustment classification for congenital heart surgery method; ICU=Intensive care unit; LOS=Length of stay; CPR=Cardiopulmonary resuscitation; ECMO=Extracorporeal membranous oxygenation; AEs=Adverse events; NA=Not applicable.
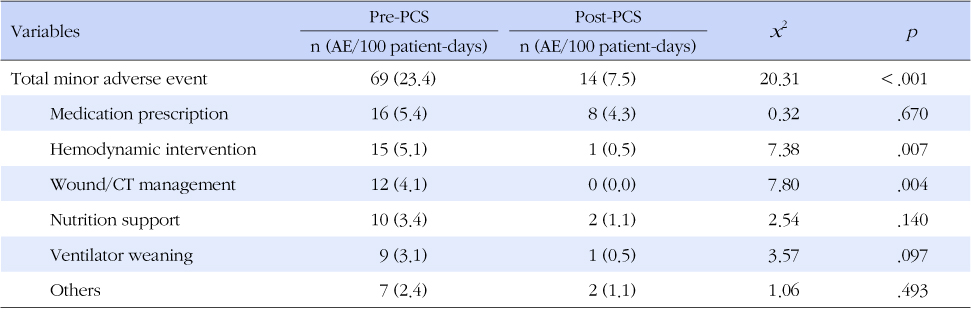
PCS=Practical communication strategies; CT=Chest tube; AEs=Adverse events.
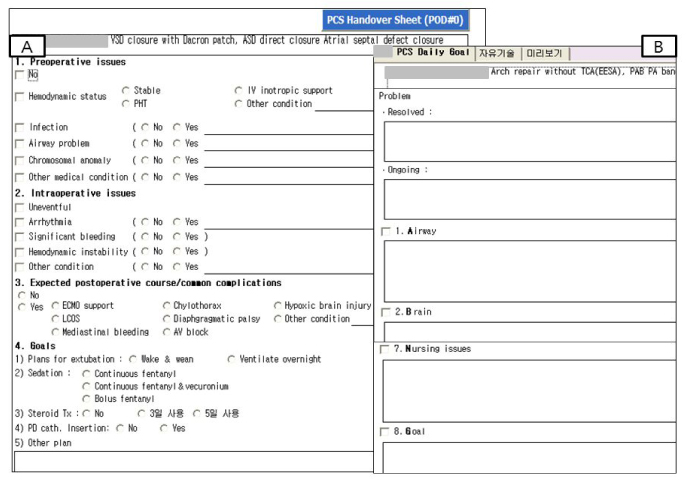
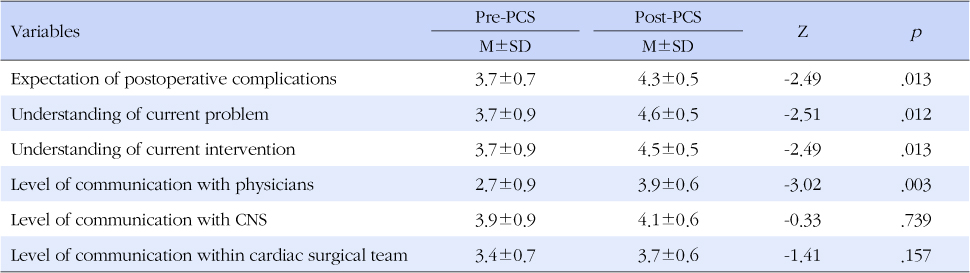
PCS=Practical communication strategies; CNS=Clinical nurse specialist.
PCS=Practical communication strategies, RACHS=Risk adjustment classification for congenital heart surgery method, CPB=Cardiopulmonary bypass, ICU=intensive care unit, LOS=Length of stay.
PCS=Practical communication strategies; RACHS=Risk adjustment classification for congenital heart surgery method; ICU=Intensive care unit; LOS=Length of stay; CPR=Cardiopulmonary resuscitation; ECMO=Extracorporeal membranous oxygenation; AEs=Adverse events; NA=Not applicable.
PCS=Practical communication strategies; CT=Chest tube; AEs=Adverse events.
PCS=Practical communication strategies; CNS=Clinical nurse specialist.