

Purpose
Nursing students are future healthcare workers responsible for maintaining public health. Owing to the increase in early resignation among new nurses, nursing education outcomes must be evaluated by investigating students' practice readiness.
Methods
Using convenience sampling, we recruited fourth-year students from two nursing colleges to participate in a cross-sectional online survey in November 2023. The Casey-Fink Readiness for Practice Survey was used to assess practice readiness and the data were analyzed using descriptive statistics, independent t-tests, and ANOVA.
Results
Among the 157 participants (female, 77.7%; mean age, 23.12±1.93 yrs), the overall practice readiness score was 63.53±8.30 (range: 20~80) and the mean subscale score was 23.14±3.73 for clinical problem-solving (range: 7~28), 6.69±1.25 for learning techniques (range: 2~8), 16.87±2.46 for professional identity (range: 5~20), and 16.82±3.46 for trials and tribulations (range: 6~24). Practice readiness did not differ significantly by gender or age and was greater among subgroups with high grades and satisfaction with the major, classroom practice, simulation practice, clinical practice, and lectures.
Conclusion
Universities must improve the quality of classes and practical education to enhance fourth-year nursing students’ practice readiness.
Nursing education programs incorporating problem-based learning must be developed and evaluated to strengthen students’ clinical inference and critical-thinking skills.
Nursing students are future healthcare workers responsible for maintaining public health. Owing to the increase in early resignation among new nurses, nursing education outcomes must be evaluated by investigating students' practice readiness.
Using convenience sampling, we recruited fourth-year students from two nursing colleges to participate in a cross-sectional online survey in November 2023. The Casey-Fink Readiness for Practice Survey was used to assess practice readiness and the data were analyzed using descriptive statistics, independent t-tests, and ANOVA.
Among the 157 participants (female, 77.7%; mean age, 23.12±1.93 yrs), the overall practice readiness score was 63.53±8.30 (range: 20~80) and the mean subscale score was 23.14±3.73 for clinical problem-solving (range: 7~28), 6.69±1.25 for learning techniques (range: 2~8), 16.87±2.46 for professional identity (range: 5~20), and 16.82±3.46 for trials and tribulations (range: 6~24). Practice readiness did not differ significantly by gender or age and was greater among subgroups with high grades and satisfaction with the major, classroom practice, simulation practice, clinical practice, and lectures.
Universities must improve the quality of classes and practical education to enhance fourth-year nursing students' practice readiness. Nursing education programs incorporating problem-based learning must be developed and evaluated to strengthen students' clinical inference and critical-thinking skills.
The Korean Accreditation Board of Nursing Education (KABNE) accredits nursing colleges throughout South Korea every 5 years, with the goal of “contributing to the improvement of national health by fostering capable nurses through continual improvement and enhancement of nursing education”[1]. This accreditation is intended to encourage self-development by determining whether nursing education is sufficient to foster nurses' capability to perform their duties at a certain level and by having educational institutions persistently evaluate their own educational conditions and programs [1]. Thus, this accreditation reflects perceptions of the importance of nursing education and can be viewed as an effort by all educators and nursing colleges to maintain a certain minimum level of quality.
Despite these efforts, turnover rates within the first year for new nurses entering clinical practice in South Korea have been growing annually, at 20.8% in 2020, 25.8% in 2021, and 28.5% in 2022 [2, 3, 4]. The main cause of this social issue is transition shock and the resulting maladaptation when unprepared nurses encounter complex clinical working environments [5]. Transition shock refers to individual experiences of doubt, confusion, loss of direction, and uncertainty caused by shifts in their roles, relationships, knowledge, and responsibilities during a change in their role or environment [6]. After graduating from nursing college, new nurses have a high rate of transition shock due to various factors, including uncertainty in their environment and interpersonal relationships, not being precisely aware of their roles, and the experience, higher expectations, and even bullying behavior of more senior colleagues [7, 8]. High transition shock places new nurses in a highly sensitive state [9], which leads to a loss of passion for learning and a change of direction, thereby increasing clinical nursing errors and adverse effects [7, 10].
Recently, the concept of nursing practice readiness has been used as a predictive factor for how successfully new nurses will adapt and how well they will perform nursing work after starting a new job [11]. Casey et al. [12] described readiness for practice as showing competence and possessing the knowledge, skills, and clinical judgment required to successfully perform one's role. Mirza et al. [13] published a concept analysis of readiness for practice, and identified the three pre-existing factors of maturity of the student, clinical practice experience, socialization into the discipline of nursing, and three interrelated properties of readiness for practice, which were cognitive capability (problem-solving skills), clinical capability (psychomotor skills, clinical assessment skills, communication skills), professional capability (feelings of self-esteem), and self-efficacy. Baumann et al. [14] performed an integrative literature review and identified four characteristics relating to nursing college graduates' practice readiness: personal characteristics (ability to manage daily tasks and workplace challenges), clinical characteristics (competency, problem-solving, decision-making), relational characteristics (communication, collaboration, teamwork), and organizational acuity (workplace awareness). New nurses with low nursing practice readiness experience difficulties applying their nursing knowledge to their job, maladaptation to their environment due to the resulting stress, and poor results in nursing tasks [13]. Thus, if the curriculum at nursing colleges were to send nurses into a clinical setting with better practice readiness, it likely would allow new nurses to rapidly adapt to their work without experiencing the transition shock that can be caused by gaps between education and practice, reduce burnout due to maladaptation, and lower the ever-growing turnover rate for new nurses [15, 16].
Nursing practice readiness is related to capabilities related to the clinical work of nurses; thus, practice readiness in fourth-year nursing students before graduation is important to investigate. Recent research has attempted to validate instruments for measuring practice readiness in nursing students [17] or new nurses [18]; however, studies investigating nursing practice readiness among senior nursing students who will soon graduate and begin working in clinical settings remain scarce. Currently, with maladaptation and early resignation among new nurses emerging as important social issues, the outcomes of nursing college education in South Korea need to be evaluated by investigating readiness for practice among senior nursing students, and the areas where they may require additional educational support. Thus, the purpose of this study was to investigate nursing practice readiness among senior nursing students and provide basic data to design measures that can help increase nursing students' readiness for practice. We aimed to contribute to establishing the essential foundation for preventing turnover among new nurses and providing safer and more effective healthcare services.
We performed a cross-sectional, descriptive study to investigate the readiness for practice among senior nursing students.
The target population for this study was fourth-year nursing students in South Korea. The participants were students at either A- University or B- University. KABNE certified the undergraduate Nursing programs at both universities in 2019 and 2020, respectively. Thus, these universities provide nursing education at or above the standards of the assessors. The specific inclusion criteria for participants were established based on a previous study [17] and are as follows: (1) Individuals currently enrolled as fourth-year nursing students and aged between 20 and 30 years. (2) Individuals who voluntarily agreed to participate after receiving detailed explanations about the purpose and procedures of the study.
For general characteristics, we included gender, age, fourth-year first-semester grades, satisfaction with major, and satisfaction with nursing education. To assess satisfaction with nursing education, we investigated satisfaction with classroom practice, simulation, clinical practice, and lectures. The questions on satisfaction were answered using a 4-point Likert scale consisting of “very satisfied,” “satisfied,” “dissatisfied,” or “very dissatisfied.”
Readiness for practice was measured using the Korean Version of Readiness for Practice Survey (K-RPS), which was adapted and validated by Lee et al. [17] from the Casey-Fink Readiness for Practice Survey (CRPS). Originally, CRPS developed by Casey et al. [12] to measure confidence/comfort in practice readiness and performance of major nursing skills in students close to graduating from nursing college. In this study, from the questions in the original questionnaire, we selected self-report questions on nursing students' confidence/comfort related to practice readiness. Casey et al. [12] verified the content and construct validity of the instrument with a panel of clinical professors. Exploratory and confirmatory factor analyses were then used to verify the construct validity with fourth-year nursing college students. This instrument consists of 20 questions across four subscales: clinical problem-solving (7 items), learning techniques (2 items), professional identity (5 items), and trials and tribulations (6 items). Each question was rated on a 4-point Likert scale (“strongly disagree”=1 point to “strongly agree”=4 points), and total scores ranged from 20 to 80 points. Higher scores indicated more confidence and comfort in one's own practice readiness, corresponding to higher nursing practice readiness.
Four questions (Q4, Q5, Q8, and Q9) were reverse scored: “I have difficulty documenting care in the electronic medical record,” “I have difficulty prioritizing patient care needs,” “I feel overwhelmed by ethical issues in my patient care responsibilities,” and “I have difficulty recognizing a significant change in my patient's condition.”. In the original development of the instrument, the Cronbach's α values for the subfactors ranged from .50 to .80, with an overall reliability of .69 [12]. In this study, the overall Cronbach's α was .88.
Data were collected in November 2023. We created an online questionnaire consisting of a research description and questions and then conducted a preliminary survey with ten fourth-year students at A- University to confirm that they had no difficulties reading the questionnaire and understanding the questions. We recruited participants by making a “research participant recruitment” post on an online message board for fourth-year students at both universities. We first explained the study's purpose, methods, and principles of voluntary participation. If they understood the purpose of the study and wished to participate voluntarily, students were asked to fill out a consent form online and participate in the survey. Participants who completed the survey were given a small token (dessert coupon) of appreciation.
We used SPSS 28.0 to analyze the data. To investigate participants' characteristics, we analyzed descriptive statistics, including the frequency, percentage, mean, and standard deviation for all questions. Differences in readiness depending on participant characteristics were analyzed using independent t-tests and one-way analyses of variance (ANOVAs). Scheffé's test was used for post-hoc analysis.
This study was approved by the Institutional Review Board of the investigators' institution (IRB No. WS-2023-41). To provide ethical protection to the participants, the study's purpose and methods and the principles of voluntary participation, including free withdrawal of consent and no penalty for not participating in the study, were explained on the participant information sheet. After receiving this information, the participants were asked to indicate their voluntarily participation in the study by completing the online consent form. No personally identifiable information such as names and telephone numbers were collected, and all participant data were encrypted and stored on a locked personal computer.
The mean age was 23.12±1.93 years and 122 were female participants (77.7%). Of the participants, 71 (45.2%) had a grade point average of 3.5~3.9 in the first semester of their fourth year. Further, 147 participants (93.7%) reported that they were more than “satisfied” with their major. Most participants were “satisfied” or better with their classroom practice, simulation practice, clinical practice, and lectures (Table 1).
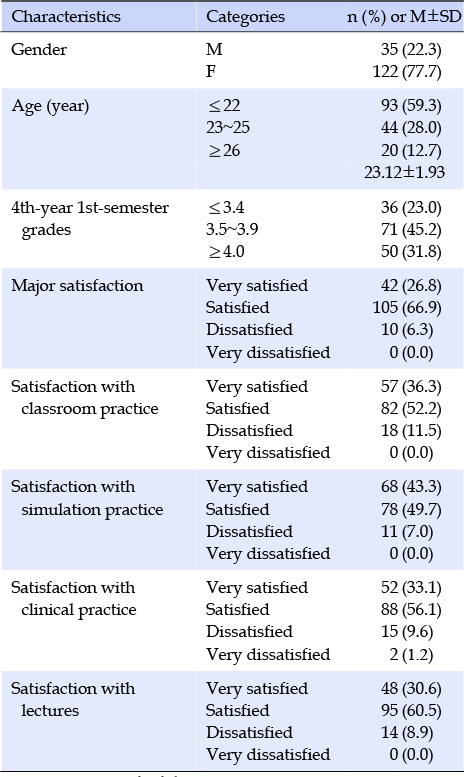
Table 1
General Characteristics (N=157)
The participants had a mean total readiness for practice score of 63.53±8.30. The questions with the highest scores were “I am comfortable delegating tasks to the nursing assistant.” (3.48±0.64) and “I have had opportunities to practice skills and procedures more than once.” (3.48±0.63). Conversely, the lowest scores were for “I feel overwhelmed by ethical issues in my patient care responsibilities” (2.19±0.87), and “I have difficulty documenting care in the electronic medical record” (2.45±0.98; Table 2).
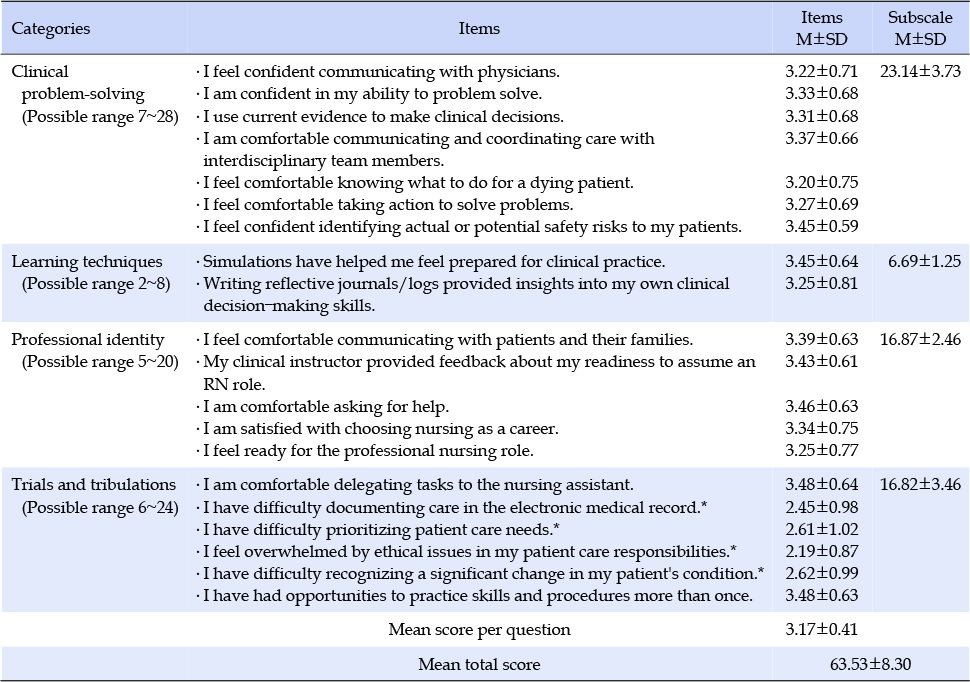
Table 2
Readiness for Practice (N=157)
The subscale scores were 23.14±3.73 for clinical problem-solving, 6.69±1.25 for learning techniques, 16.87±2.46 for professional identity, and 16.82±3.46 for trials and tribulations (Table 2).
Our analyses based on participant characteristics showed no significant differences in practice readiness depending on gender (t=-0.28, p=.778) or age (F=0.40, p=.670). However, significant differences were found in readiness for practice depending on fourth-year first-semester grades (F=8.16, p<.001) and satisfaction with major (F=11.52, p<.001), classroom practice (F=7.69, p<.001), simulation practice (F=10.76, p<.001), clinical practice (F=4.45, p=.005), and lectures (F=4.42, p=.014). Specifically, readiness for practice was higher among students with a grade point average of 4.0 in the first semester of their fourth year compared to those with averages ≤3.4. Practice readiness was also higher among students who were “very satisfied” with their major, classroom practice, or simulation practice, compared with those who were “satisfied” or “dissatisfied.” Students who were “very satisfied” with clinical practice or lectures showed higher readiness for practice than those who were “satisfied”(Table 3).
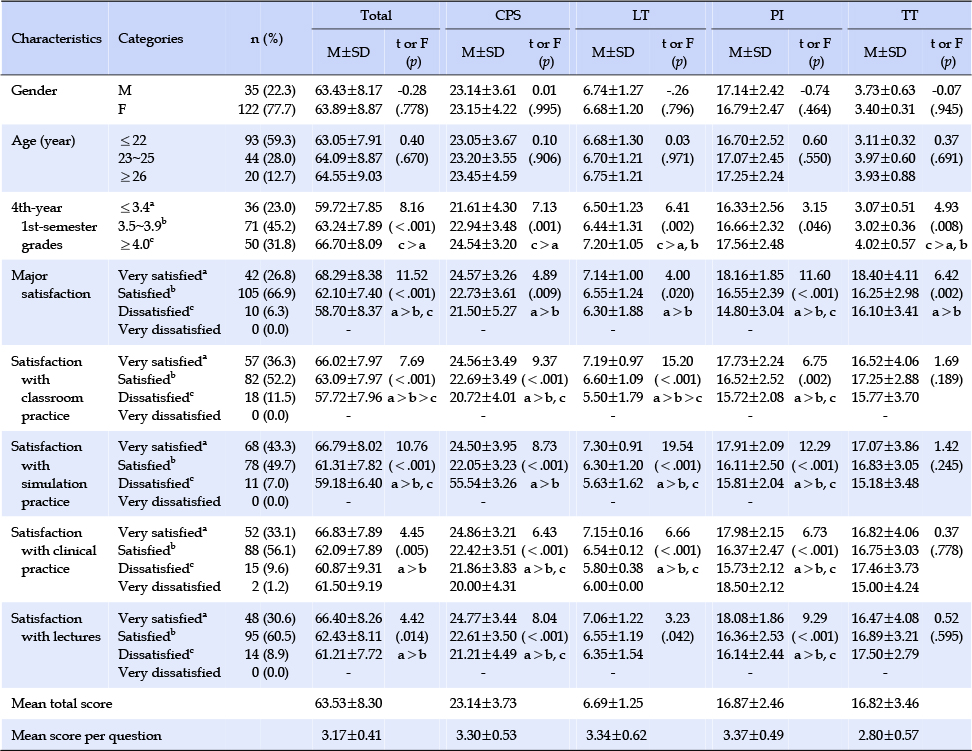
Table 3
Differences in Readiness for Practice according to the Participants' Characteristics (N=157)
There were no differences in the subscales of clinical problem-solving, learning techniques, professional identity, and trials and tribulations based on the participants' gender and age. In the subscales of clinical problem-solving, learning techniques, and professional identity, significant differences were observed based on fourth-year first-semester grades, satisfaction with the major, classroom practice, simulation practice, clinical practice, and lectures. However, in the subscale of trials and tribulations, significant differences were found based on fourth-year first- semester grades and satisfaction with the major (Table 3).
We investigated senior nursing students' readiness for practice, to evaluate the outcomes of current nursing college education, and to identify areas needing further educational support. The purpose for conducting this study was to ultimately explore measures to reduce transition shock for nurses working in clinical settings after graduation, thereby increasing successful organizational adaptation and decreasing turnover rates.
In this study, fourth-year nursing students had a mean readiness for practice score of 63.53 points, on a scale ranging from 20 to 80 points. Ersoy and Ayaz-Alkaya [19] validated the same instrument in another country, and with 15 total questions, the mean score of fourth-year nursing students was 46 points on a scale ranging from 15 to 60 points. However, the difference in the number of questions makes direct comparisons difficult. Further research will be needed to determine a cutoff score for evaluating the outcomes of nursing college education.
When we considered individual questions, the mean scores of those on the trials and tribulations subscale were in the range of 2.19±0.87 to 2.62±0.99, which was lower than the mean scores for items on the other subscales. The trials and tribulations subscale includes questions about setting priorities for patient care, writing electronic medical records (EMR), ethical dilemmas, and detecting changes in patients' conditions. In these situations, nurses must make decisions based on the environment and the patient's status, without any definite answers. Senior nursing students lack work experience and are therefore likely perceive the highest level of difficulty regarding readiness for practice in challenging situations. In a previous study, Mollart et al.[20], found that most third-year nursing students had only learned paper-based documentation, which left them feeling unprepared to use EMR in a clinical setting and lacking confidence about approaching EMR. This demonstrates the need to provide opportunities for nursing students to use EMR programs. Most students first encounter EMR programs during clinical practice; however, this is typically limited to observation, owing to issues with protecting personal information. Schools need to provide EMR programs designed for practice to improve students' understanding of EMRs and reduce their fear. New nurses require education and feedback about prioritizing work responsibilities situationally, improving their ability to solve patients' problems, and dealing with ethical dilemmas. Currently, nursing students generally have suitable access to simulation practice, which is part of the curriculum at most nursing colleges. In clinical settings, nursing students have limited opportunities to act autonomously; thus, simulation practice rooms provide a constant environment for students to repeatedly perform the role of a nurse, receive education and feedback on situationally prioritizing work, improve their ability to solve patients' problems, and learn to handle ethical dilemmas.
In this study, there were no differences in readiness for practice based on gender and age among senior nursing students, which is consistent with the findings of Jang and Mo [21]. This suggests that individual characteristics and experiences of nursing students have a greater influence on readiness for practice than biological differences such as gender and age. In other words, factors such as the curriculum quality, availability of clinical opportunities, and the attitudes of individual students have a more significant impact on readiness for practice, and support should be provided to ensure these factors play a crucial role.
In our study, the subgroups with high grades and high satisfaction with their major showed higher readiness for practice. Grades and satisfaction with one's major have been shown to be related to achievement motivation [22]; therefore, we posit that the subgroups with high grades and high satisfaction with their major also have high achievement motivation, which may have contributed to their high readiness for practice. However, low satisfaction with major is an obstacle for the formation of proper attitudes to efficiently performing nursing work and the formation of positive professional values when students later become nurses [23]. Multiple approaches are needed to improve students' satisfaction with their major. Providing opportunities for in-depth study in various specialized fields (such as psychiatric nursing, pediatric nursing, and cardiac nursing) allows students to explore their areas of interest, thereby enhancing their satisfaction with the major. Additionally, the curriculum and learning environment should be practice-oriented to stimulate students' interest in the field. Nursing universities should establish collaborative relationships with hospitals to offer mentoring programs, field visits, and internship opportunities, enabling nursing students to gain essential skills and experience in real-world clinical settings.
In our study, the subgroups showing high satisfaction with classroom, simulation, and clinical practice also showed higher readiness for practice. This demonstrates the importance of the quality of practical education for educational outcomes related to practice readiness at nursing colleges. Classroom practice, such as basic nursing and health identification practice, which are typically classes taken in students' second year, is part of the process of acquiring basic practical skills using nursing knowledge and preparing for clinical practice. These experiences are also students' first with practice in the area of their major, and the educational and psychological outcomes of classroom practice education can affect later clinical practice outcomes [24]. Although students often feel “a sense of achievement and pride” after basic nursing practice, they may also have thoughts such as, “as a nurse, I feel less confident about my growth” [25]. Decreased confidence in nursing after classroom practice can affect clinical practice and readiness for practice. Thus, while also focusing on improving students' nursing skills, practical instructors must implement teaching methods that encourage self-confidence in nursing.
Further, the participants in this study experienced limited in-person practice due to COVID-19, often taking remote practical lessons online. Thus, they lacked opportunities to practice their skills intensively, and this context should be considered when interpreting our findings. Factors that can affect the educational outcomes of practical classes provided online include aspects of class management, such as the content and implementation methods, and students' personal characteristics, such as degree of practical participation, self-learning ability, learning confidence, and self-efficacy concerning online learning [26, 27]. Experts are warning that new infectious diseases that could cause another situation similar to the COVID-19 pandemic will continue to emerge and the time between outbreaks will become shorter [28, 29]. Thus, exploring measures to overcome the limitations of online practice as a replacement for in-person practice and improving the quality of practice education are imperative to achieving equivalent learning outcomes through developing effective online content and integrating different disciplines.
In our study, the subgroup with very high satisfaction with simulation practice showed higher readiness for practice than other subgroups. Nursing students' opportunities to perform nursing tasks directly during clinical practice have declined due to stronger awareness of patient rights and problems with patient safety. To overcome these limitations, the importance of simulation education has been increasingly emphasized, as it can provide students with experience in diverse clinical scenarios in realistic environments. Thus, simulation education can help solve the ethical issues of practicing directly on patients, while increasing patient safety and reducing errors, and the process of transferring theoretical knowledge to actual practice can improve nursing competencies such as problem-solving, critical thinking, clinical performance, communication, and self-leadership [30]. Ragsdale and Schuessler [31] reported that simulation could improve readiness for practice in graduating senior nursing students via effects on preparation (learning experience, self-confidence), competence development (communication and documentation), clinical reasoning, and the number of human patient simulators for the experience. Therefore, nursing colleges should make efforts to improve the quality of simulation practice using the diverse equipment at their disposal. In addition to the use of high-fidelity simulators and standard patients, spatial and temporal restrictions can be resolved by developing and using realistic, highly interactive simulation programs using web-based methods (Virtual Simulation for Nursing, vSim [32]), augmented reality [33], and virtual reality [34].
In our study, the subgroup with very high satisfaction with clinical practice also showed higher readiness for practice. In a study of new nurses, Kim [35] identified satisfaction with clinical practice as a factor affecting readiness for practice, confirming the importance of clinical practice. Clinical practice allows nursing students to experience a hospital setting as reality, connecting theory and practice, empathizing with patients, improving motivation and self-esteem, and preparing for the future [36]. Nursing is a practical discipline, and nursing students experience diverse situations and emotions during clinical practice, learning, and preparing for their roles as nurses. However, the founding of new nursing departments and rapid increase in the number of students has outpaced the number of hospitals offering practical experience, leading to a decline in the quality of clinical practice, which has lowered students' satisfaction with clinical practice. Owing to the issue of low birth rates, pediatric nursing practice and maternity nursing practice have suffered substandard allocation of practical locations. As a solution, KABNE has allowed clinical practice to be replaced with simulation practice; thus, it will be important to improve the quality of simulation practice so that it can have similar or better educational effects than clinical practice.
In our study, the subgroup with high satisfaction in theoretical education showed higher readiness for practice, which demonstrates the importance of the quality of theoretical education. Since nursing is a discipline with a scientific body of knowledge applied to practical work, education in nursing theory is also important. The lecture-based educational methods typically used in nursing theory allow a large amount of subject-specific content to be delivered effectively through lessons that aim to convey conceptual knowledge. However, there are limitations with regard to expanding learners' thinking, improving problem-solving abilities, and teaching efficient communication [37]. Regarding pedagogy, student-participatory education has been found to be more effective than lecture-based education [38], and it will be important to stimulate student participation by shifting the focus of learning from instructor-centric to student-centric learning. Various pedagogical methods could be employed, such as flipped learning, blended learning, or problem-based learning. In addition, classes using case-based learning and inferential reading can improve communication and self-directed learning abilities in nursing students [39], which could increase readiness for practice.
This study is valuable because we investigated the readiness for practice of senior nursing students and suggested measures to improve readiness for practice. Nevertheless, this study had several limitations. First, because we collected data by convenience sampling among students at two nursing colleges, caution is required when generalizing the interpretations of our findings. We suggest that replication studies be conducted in the future using a sample with a broader representation. Second, because we investigated readiness for practice using a self-report questionnaire, the results could have been affected by social desirability bias. The participants could have given subjectively or socially appropriate responses, irrespective of their actual readiness. In the future, in addition to selfevaluation methods, it will be important to include objective evaluations of readiness for practice by instructors. Finally, when our findings are compared with other studies, it will be important to consider the context, since the participants in our study took online replacement practice classes during the COVID-19 pandemic in 2021, and thus had a limited actual practice experience. There are limitations in treating our results as the standard for readiness for practice among senior nursing students in South Korea.
In our study, the mean total readiness for practice score of senior nursing students in South Korea was 63.53 points, and the score for the Trials and Tribulations subscale was lower than the mean of other subscales. In addition, we observed significant differences in readiness for practice depending on grades, satisfaction with major, satisfaction with classroom practice, satisfaction with simulation practice, satisfaction with clinical practice, and satisfaction with theoretical lectures. This demonstrates the need for strategies that can increase satisfaction with major, classroom practice, simulation practice, clinical practice, and theoretical lectures in order to improve readiness for nursing practice among senior nursing students. It will be necessary to first identify nursing students' educational needs, to regularly evaluate the quality of all curricula, and to provide high-quality education, to improve students' problem-based learning, clinical inference, and critical thinking abilities. By applying diverse pedagogical methods, such as flipped learning, blended learning, or problem-based learning, students' active participation can be encouraged, maximizing the learning effect. In addition, detailed simulation practice, which can compensate for the limitations and shortcomings of clinical practice through realistic clinical scenarios and a high level of interactions, can be used to increase students' satisfaction and improve readiness for practice. In the future, it will be important to conduct replicate studies on readiness for practice that account for different regions and educational environments, and we also propose qualitative research on nursing students' readiness for practice. We suggest that interventional studies should be conducted, developing, implementing, and validating nursing education programs that can improve readiness for practice based on these findings.
Source of research fund or grant: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. RS-2022-00165947).