

Purpose
This qualitative study explored nurses' experiences in selecting hospitals within a dual labor market framework.
Methods
Focus group interviews were conducted with 18 general nurses, divided into three groups of six, each representing both large and medium-sized hospitals.
Results
The analysis revealed two themes, four categories, and nine subcategories, highlighting differences between large and medium-sized hospitals. Nurses who choose large hospitals prioritized "professional development" but faced "struggles to maintain professional identity" while those selecting medium-sized hospitals sought "stability and accessibility" but experienced "crisis of professional identity." Conclusion: This study highlights significant differences in the factors influencing nurses' hospital choices based on hospital size. These findings provide foundational data for establishing the Enforcement Decree and Rules of the Nursing Act, emphasizing the importance of developing legal measures to strengthen nurses' professional identity and promote a balanced and sustainable nursing labor market.
This qualitative study explored nurses' experiences in selecting hospitals within a dual labor market framework.
Focus group interviews were conducted with 18 general nurses, divided into three groups of six, each representing both large and medium-sized hospitals.
The analysis revealed two themes, four categories, and nine subcategories, highlighting differences between large and medium-sized hospitals. Nurses who choose large hospitals prioritized “professional development” but faced “struggles to maintain professional identity” while those selecting medium-sized hospitals sought “stability and accessibility” but experienced “crisis of professional identity.”
This study highlights significant differences in the factors influencing nurses' hospital choices based on hospital size. These findings provide foundational data for establishing the Enforcement Decree and Rules of the Nursing Act, emphasizing the importance of developing legal measures to strengthen nurses' professional identity and promote a balanced and sustainable nursing labor market.
The global nursing shortage remains a pressing issue for healthcare systems, with significant consequences extending beyond individual institutions to national health policies. In South Korea, small- and medium-sized hospitals face particularly acute challenges in retaining nursing staff. High turnover rates in these hospitals contribute to operational instability, declining healthcare quality, increased patient safety risks, and escalating healthcare costs [1]. Efforts to mitigate the nursing shortage in Korea have included substantial increases in nursing education capacity, with admission quotas in regional nursing colleges nearly doubling from 11,686 in 2008 to 23,883 in 2024 [2, 3]. However, the anticipated improvements have been limited. Only 50% of licensed nurses actively practice, and the annual turnover rate among nurses remains alarmingly high at 15.2%-approximately three times that of other healthcare professions [4, 5]. Turnover rates are disproportionately higher in smaller hospitals, with tertiary hospitals reporting a relatively low rate of 11.6% compared to 20.0% in general hospitals and 17.3% in small hospitals. Among small hospitals with 200~399 beds, turnover rates reach 24.6%, nearly 2.6 times higher than those observed in hospitals with over 1,000 beds [3]. These disparities underscore the structural inequities inherent in the nursing labor market, which influence not only retention rates but also employment decisions across different types of hospitals.
The dual labor market theory, introduced by Doeringer and Piore in the 1960s, provides a conceptual framework for understanding these challenges. This theory posits that labor markets are segmented into primary and secondary sectors, characterized by distinct employment conditions. The primary sector offers higher wages, stable employment, and opportunities for career advancement, while the secondary sector is marked by low wages, precarious employment, and limited mobility [6]. Within the nursing profession, large hospitals typically align with the characteristics of the primary labor market, providing competitive wages, stable working environments, and professional development opportunities. In contrast, small and medium-sized hospitals are emblematic of the secondary labor market, offering less favorable conditions that exacerbate turnover rates and workforce shortages [7]. These structural divisions highlight how employment decisions among nurses are shaped by the contrasting characteristics of primary and secondary labor markets, reflecting broader systemic inequalities in the nursing workforce.
According to a systematic review of nurses' turnover, numerous studies focus on individual and organizational factors such as workload intensity, inadequate compensation, and unsatisfactory working conditions [8]. However, these studies often fail to account for the structural disparities inherent in the dual labor market, particularly the contrasting dynamics of large versus small hospitals. Moreover, the increasing reliance on cost-efficiency measures in large hospitals-such as reduced inpatient length of stay and expanded integrated nursing care services-has further intensified the demand for nursing staff, deepening structural imbalances and drawing resources away from smaller hospitals [9].
Addressing these disparities requires a nuanced understanding of the dual labor market's impact on nurses' employment decisions. Such an approach can inform targeted policy interventions that address the unique needs of small hospitals while alleviating structural imbalances within the nursing labor market.
This study explores nurses' experiences in hospital selection through the lens of dual labor market theory, aiming to provide actionable insights to address staffing shortages in smaller hospitals. Furthermore, the findings aim to inform the development of legal measures under the recently enacted Nursing Act, contributing to structural reforms that promote equity and sustainability in the nursing labor market.
This qualitative study utilized focus group interviews (FGIs) to investigate nurses' experiences with hospital selection within the framework of dual labor market theory. FGIs were chosen for their ability to capture diverse perspectives and promote reflective dialogue among participants with similar or differing experiences [10].
The participants of this study were general nurses employed in healthcare institutions. To investigate hospital selection within the dual labor market framework, the participants were selected based on the structural segmentation of small and large hospitals. The classification of hospitals was guided by prior empirical analyses, which identified hospitals with 500 or more beds as large hospitals and those with fewer than 500 beds as small hospitals [7]. The inclusion criteria for participant selection were as follows:
• Nurses who transitioned between large and small hospitals.
• Nurses who continuously worked in either large or small hospitals.
Participants were recruited through announcements on social media, which included details on the study's purpose, participation methods, schedule, and benefits. Following the FGI standards outlined by Krueger and Casey [10], each focus group aimed to include 6~10 participants. A total of 18 participants were recruited, and three FGI groups were formed, each composed of 6 nurses from both small and large hospitals to ensure diverse perspectives within each group. Among the participants, 15 were female, and 3 were male, with an average age of 28.1 years and clinical experience ranging from 1 to 9 years. Six participants had prior job transition experience, while 12 had not. Additionally, 10 participants were employed in large hospitals, and 8 were employed in small hospitals (Table 1).
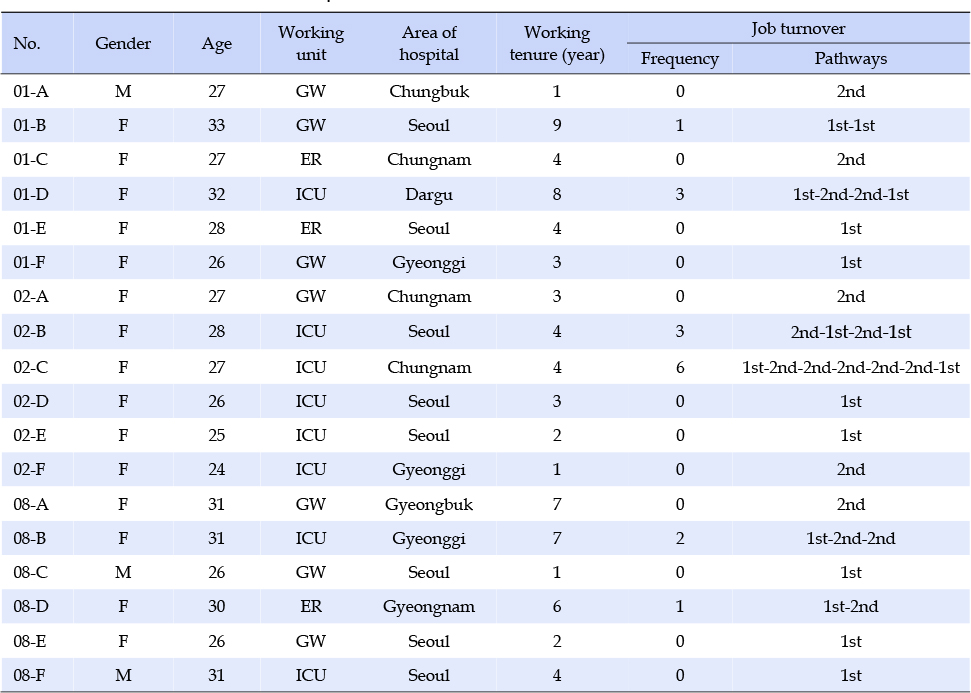
Table 1
General Characteristics of Participants
Data were collected over a one-week period from December 1 to December 8, 2021 through Focus Group Interviews. The interview protocol was systematically developed following Krueger and Casey's framework [10], which delineates four phases: introductory, transition, key, and concluding questions. An expert panel comprising three nursing professors and three practicing nurses rigorously reviewed the interview guide to ensure clarity, relevance, and alignment with the study objectives. The finalized questions are presented in Table 2.
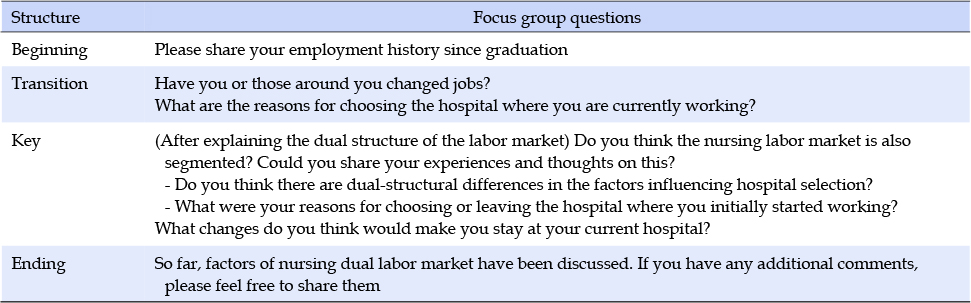
Table 2
Questions for a Focus Group Interview (FGI)
Each FGI session involved three researchers with distinct roles to ensure methodological rigor. The lead facilitator guided discussions, ensuring alignment with the research objectives, while the assistant documented group dynamics, nonverbal expressions, and maintained detailed field notes. The observer focused on capturing nuanced interactions and reflective insights to enrich the data analysis. To promote balanced participation, the facilitator tactfully addressed any dominance or off-topic discussions, with such interventions recorded in the field notes. A conducive environment fostered open and honest sharing, and probing questions facilitated richer, in-depth responses. Sessions concluded with member checking to ensure the trustworthiness of interpretations and to allow participants to provide additional insights.
FGIs were conducted until data saturation was achieved, with no new themes or insights emerging. All sessions were audio-recorded with the informed consent of participants. Following each session, the research team compiled detailed debriefing notes to capture significant observations and emergent themes. The final data corpus included audio recordings, verbatim transcripts (128 pages), field notes, and debriefing notes. This comprehensive dataset and the collaborative efforts of the three researchers contributed to the methodological rigor, ensuring the dependability and credibility of the findings.
The rigor of this study was ensured using Lincoln and Guba's trustworthiness framework. Credibility was established by purposefully recruiting participants with relevant experiences, fostering open communication during focus group interviews, and using member checking to align researcher interpretations with participants' intended meanings. Audio recordings were cross-checked with transcripts to ensure accuracy. Dependability focused on the consistency and traceability of the research process, achieved through meticulous documentation of the study's rationale, objectives, and methods. An audit trail enabled external reviewers to trace the research process, and collaborative data analysis ensured reliability. Direct participant quotations illustrated the linkage between raw data and findings. Transferability assessed the applicability of findings to other contexts. Participants from diverse backgrounds were recruited through open online announcements based on predefined criteria, and data collection continued until saturation was reached. External nurses reviewed the findings, validating their relevance to professional experiences. Confirmability ensured findings were data-driven and free from researcher bias. Reflexivity was maintained through documented preconceptions and team discussions. The research team regularly reviewed data collection, audit trails, and analytical procedures to confirm alignment with participants' narratives. Adherence to these criteria ensured the trustworthiness of the qualitative findings.
The data analyzed in this study included FGI transcriptions and field notes documented by the researchers. Three experienced qualitative researchers conducted the analysis using Graneheim and Lundman's framework [11]. They independently reviewed the transcripts multiple times to immerse themselves in the data and identify significant words, phrases, or sentences related to hospital selection. These were condensed into meaning units, organized in Microsoft Excel, and abstracted into codes capturing key concepts. The codes were compared for similarities and differences, grouped into subcategories, and then clustered into broader categories based on shared meanings. Through iterative discussions, categories were synthesized into overarching themes, continuing until data saturation was achieved, marked by the absence of new codes or categories.
A total of 9 subcategories were grouped into 4 categories and refined into 2 main themes. Weekly team meetings ensured consistency, resolved discrepancies, and finalized category and theme names. To enhance trustworthiness, two nursing professors with qualitative research expertise externally reviewed the categories and themes. Their feedback on representativeness and exclusivity was incorporated into the final analysis, ensuring the findings accurately reflected nurses' hospital selection experiences.
This study was approved by the Institutional Review Board (IRB) of Andong National University (Approval No. 1040191-202109-HR-020-01). All procedures adhered to the ethical guidelines established by the IRB. Participants provided informed consent through electronically signed forms before the interviews. The consent form detailed the study's purpose, procedures, methods of data collection (including audio recording), plans for data usage and storage, potential risks, and benefits, along with assurances of voluntary participation. Participants were informed that they could withdraw from the study at any time without consequences, and all collected data would be used solely for research purposes.
To ensure confidentiality and anonymity, all identifiable information was coded during transcription. The transcripts and analysis materials were securely stored on password-protected personal computers accessible only to the researchers. These precautions ensured compliance with ethical standards for data protection and confidentiality. Furthermore, researchers maintained a neutral stance during data collection and analysis, minimizing bias and respecting participants' autonomy. All research materials, including recordings and field notes, will be retained for a specific duration as required by institutional policies and will be securely deleted afterward.
The findings of this study, grounded in the dual labor market theory, revealed two primary themes regarding nurses' hospital selection experiences: “The dual structure in choosing hospitals” and “The dilemma of professsional identity”.
This theme highlights the distinct factors influencing hospital selection among nurses employed in large hospitals (primary labor market) versus small and medium-sized hospitals (secondary labor market). The findings were categorized into two primary categories: “Choosing for professional development” and “Choosing for stability and accessibility”. (Table 3)
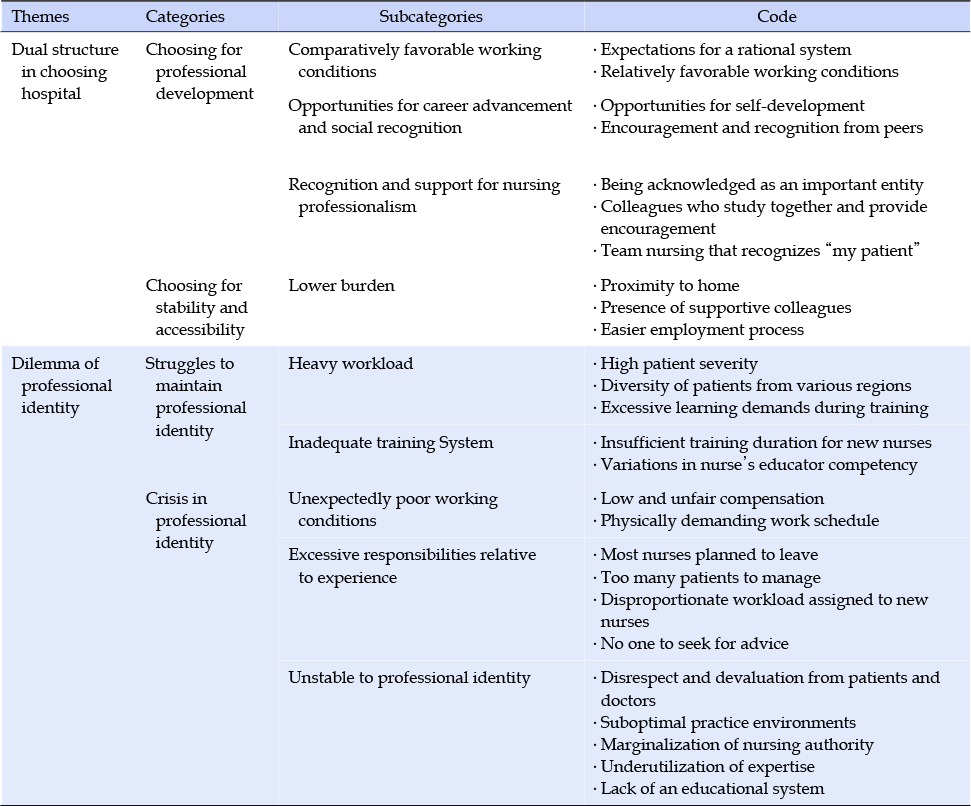
Table 3
Dual-Structural Differences in Factors Influencing Hospital Selection and Turnover
This category captures the factors motivating nurses in large hospitals to select their workplaces. It includes three subcategories: “Comparatively favorable working conditions”, “Opportunities for career advancement and social recognition”, and “Recognition and support for nursing professionalism”.
This subcategory highlights the compromises participants made in choosing large hospitals. Nurses were drawn by “Expectations for a rational system” and “Relatively favorable working conditions.” Participants perceived large hospitals as having better-organized schedules and performance-based reward systems compared to small hospitals. However, this was often seen as a relative advantage rather than an ideal condition, with some nurses expressing a lack of long-term commitment to the profession.
Compared to regional hospitals, I thought I might be evaluated more based on my performance… and possibly receive better rewards. (01-B)
I considered working near home because this job is exhausting, but my friends told me… small hospitals require back-to-back shifts that last longer than those at large hospitals. It sounded too challenging. (02-D)
The salary here is lower than other university hospitals, but at least the off-days are guaranteed. It's not great, but it's why I'm still here. (02-B)
If I continue working in clinical settings, I doubt I'll move hospitals. I don't think I'll find a place that satisfies me. (02-E)
This subcategory includes “Encouragement and recognition from peers” and “Opportunities for self-development.” Participants noted that the reputations of large hospitals and societal expectations influenced their decisions. The exposure to diverse clinical cases and ample training opportunities made large hospitals appealing for long-term career development.
I wanted to see a variety of cases… my seniors often said it's better to start at a large hospital because transitioning from a small to a large hospital is much harder. (08-F)
I prioritized educational opportunities over salary. Even though living expenses in Seoul are high, the chance for personal growth made it worthwhile. (01-B)
This subcategory includes “Being acknowledged as an important entity,” “Colleagues who study together and provide encouragement,” and “Team nursing that recognizes ‘my patient.’” Participants felt that large hospitals recognized their expertise and integrated them as critical members of the healthcare team. Collaborative peer support and structured nursing systems, such as team nursing, reinforced their professional identity and pride.
It's an environment where I can focus solely on nursing. I truly felt like a nurse contributing to patient care, supported by a system that recognized my role as part of the medical team. (01-B)
In my unit, we have study groups, and the hospital supports us with resources. This makes it easier to adapt and feel motivated. (02-D)
Team nursing allowed me to have my assigned patients regardless of my experience level. It gave me a sense of responsibility and professionalism. (01-F)
This category captures the motivations of nurses who opted to work in small- to medium-sized hospitals. It includes one subcategory: “Lower burden”.
This subcategory includes three codes which are “Proximity to home”, “Presence of supportive colleagues,” and “Easier employment process.” Nurses working in small hospitals often prioritized practical considerations over professional development. Proximity to family support, connections with friends or acquaintances, and the ease of the hiring process were significant factors in their hospital choice.
It's close to home, which was the biggest reason… economically, it made sense to work nearby. The hiring process was smooth, too, which made it even easier. (01-A)
When I switched jobs, I prioritized hospitals where I had friends or people I could rely on… ideally, somewhere comfortable. (08-A)
Frequent job changes weren't really frowned upon. I guess it's because they're always short-staffed. I got lucky and was able to find jobs quickly. (02-C)
This theme highlights the shared conflicts experienced by nurses in both large and small hospitals regarding their professional identity. It encompasses two categories: “Struggles to maintain professional identity” and “Crisis in professional identity.”
This category represents the burdens that large hospital nurses bear to preserve their professional identity, often leading to thoughts of leaving their positions. It consists of two subcategories: “Heavy workload” and “Inadequate training systems.”
The subcategory “Heavy workload” reflects the overwhelming level of work demands faced by nurses in large hospitals, contributing to their intentions to resign. Participants identified factors such as “High patient severity,” “Diversity of patients from various regions,” and “Excessive learning demands during training” as contributors to this challenge.
I don't even realize how eight hours pass. With four ventilated patients, it always feels like this isn't right. If there's an event with one patient, the others are practically neglected because we're so short-staffed. (01-F)
Many patients and caregivers come from regional areas, and they often complain, saying, Why isn't this done here? Other hospitals do it. These complaints really add to the stress. (08-D)
Once I started working, I realized I knew less than 1% of what I needed. I felt so incompetent, and I spent all my time outside of work studying-before shifts, after shifts, at the library reviewing patient cases. It was an endless cycle, and I felt like my mental health was at serious risk if I stayed. (08-E)
The subcategory “Inadequate training systems” highlights deficiencies in both the duration and quality of training provided to new nurses. It includes two codes: “Insufficient training duration for new nurses” and “Variations in nurse educators' competency.” Participants acknowledged that, despite relatively structured training systems in large hospitals, the high demands often outpaced the available resources. Training durations were reported to be shortened, especially as the intake of new nurses increased. Additionally, disparities in the competencies of nurse educators led to inconsistencies in the quality of training, leaving nurses feeling underprepared and increasing their psychological burden.
The number of new nurses has increased so much that training durations have been shortened. When I started, it was three months, but now it's just about six weeks before they are assigned to patients. (01-F)
Our preceptor period is supposed to be 10 weeks, during which we handle things like CRRT and ventilators. ECMO training comes three months later, but we're thrown in knowing almost nothing and told, ‘This is how you do CRRT. It's terrifying. (08-F)
Compared to small hospitals, we have nurse educators and a somewhat structured system. In general wards, it's about an eight-week training period, and for the ICU, 10 weeks. But the content taught varies by preceptor. Some preceptors contradict others, and you end up being scolded for doing things differently. It's still really tough. (08-D)
This theme underscores the significant challenges faced by nurses in large hospitals as they navigate high workloads and insufficient training systems, often at the expense of their professional identity and well-being.
This theme highlights the challenges faced by nurses in small- and medium-sized hospitals, particularly the factors threatening their professional identity and contributing to high turnover rates. It encompasses three categories: “Unexpectedly poor working conditions”, “Excessive responsibilities relative to experience”, and “Unstable professional identity”.
This category captures the unexpectedly substandard working conditions experienced by nurses in small- and medium-sized hospitals. It includes two subcategories: “Low and unfair compensation” and “Physically demanding work schedule” Participants reported that their salaries were significantly lower than expected, with some encountering unfair compensation practices, such as unclear calculations for overtime. Additionally, they described unstable shift schedules, prolonged consecutive workdays, and an inability to take necessary leave, leading to extreme physical and emotional exhaustion.
My salary was the same as a nursing assistant's… I felt a sense of inferiority, like my degree and education meant nothing because I was treated the same. (01-D)
Even though the work hours were technically 11 hours, 2.5 hours of rest time were deducted from my overtime pay. So the night shift pay ended up being the same as regular pay. (02-F)
In a month, I had only six or seven days off. It was mostly NOD shifts, sometimes even NOP. I've worked three consecutive night shifts followed by a single day off and six evening shifts. I was sick and couldn't even rest because they'd say, ‘You're new, how can you already be sick?' (01-C)
This category reflects the overwhelming burden placed on nurses due to staff shortages and inadequate preparation. It includes four codes: “Most nurses planned to leave”, “Too many patients to manage”, “Disproportionate workload assigned to new nurses”, and “No one to seek for advice” Participants described situations where understaffing led to excessively high nurse-to-patient ratios. Many nurses working in these hospitals were awaiting assignments to larger hospitals, leading to unstable team dynamics. Furhermore, the frequent turnover of physicians left nurses without proper guidance, intensifying their anxiety.
Out of six nurses, three are waiting for their placements at other hospitals. Since they're still learning, you can see how exhausted the remaining team is. (08-A)
Even though I was completely new, I was given charge nurse duties. I was responsible for 60 patients during one shift. The workload was overwhelming, and that's why I switched to night shifts. (02-F)
I'm still a new nurse, but I get assigned critical patients while also handling admissions to the ICU. It felt like everything was on me, and it was unbearable. (08-B)
Doctors change frequently, and sometimes they don't know how to handle situations. I feel like I can't ask anyone for advice. Our head nurse has been gone for months, and the senior nurse with three years of experience is leaving soon. (02-F)
This category illustrates the factors undermining nurses' sense of professional identity, further influencing their intent to leave. It consists of five codes: “Disrespect and devaluation from patients and doctors”, “Suboptimal practice environments”, “Marginalization of nursing authority”, “Underutilization of expertise”, and “Lack of an educational system” Participants noted being disrespected by patients and doctors, as well as frequent violations of nursing standards, such as improper aseptic techniques. They also reported being asked to perform tasks beyond their scope, such as assisting with pharmaceutical duties or administrative tasks, leading to feelings of professional marginalization. The lack of a structured education system, including poorly implemented preceptor programs, left new nurses ill-prepared and unsupported.
Elderly patients often call us ‘miss’ or ‘nurse girl.’ Even when notifying doctors, I felt belittled, like this wasn't the right hospital to work at. (01-C)
Basic standards weren't followed. They reused syringes for a week and cut open IV set packaging for convenience. It made me question if I was practicing nursing properly. Even with higher pay, I couldn't stay there long. (01-D)
Nurses here have to do the work of doctors, pharmacists, and even lab technicians. I've been asked to prescribe medications, which is illegal, but it's treated as normal because the pharmacist only works four days a week. (02-C)
There's no real preceptor system. Every shift, I had to work with different nurses. It felt chaotic, like being thrown into a pool and told to learn on my own. (08-B)
This study explored the hospital selection experiences of nurses within the framework of the dual labor market structure, focusing on “The dual structure in choosing hospitals” and “Dilemma of professional identity.” These two themes serve as the foundation for this discussion.
The theme “The dual structure in choosing hospitals” highlights distinct motivations and expectations for hospital selection between nurses in large hospitals and those in small- and medium-sized hospitals, reflecting the dual structure of the nursing labor market. According to Jacobs and Brieger's dual labor market theory (1988), primary labor markets-represented by large organizations-are characterized by factors such as high wages, comprehensive benefits, job stability, favorable working conditions, career advancement opportunities, education and training, social prestige, fairness, procedural clarity, and promotion prospects [12, 13]. Similarly, this study's participants cited favorable working environments, opportunities for social recognition and career development, and support for nursing professionalism as key factors in their decision to work in large hospitals. Conversely, reasons for choosing small- and medium-sized hospitals were less focused on hospital-specific attributes and more influenced by external support systems, including family and colleagues. This aligns with findings from prior studies, where nurses transitioning to smaller hospitals sought lower expectations and stable, long-term employment [14].
However, the distinct characteristics of the nursing labor market demand tailored strategies beyond the dual labor market framework. Addressing imbalances in staffing and retention requires interventions that account for structural disparities. In large hospitals, reducing workload intensity and enhancing career pathways are essential to sustaining their appeal as primary labor markets [15]. In small hospitals, policies must focus on improving job stability, equitable compensation, and localized career development. Initiatives such as flexible scheduling, peer-support programs, and family-friendly policies can provide psychological and social support valued by nurses in secondary labor markets.
The theme “Dilemma of professional identity.” underscores the significant burdens faced by nurses in maintaining their professional identity. Nurses in large hospitals reported high levels of stress stemming from complex patient needs, heavy workloads, and demanding learning requirements. Participants emphasized the need for improved educational frameworks to mitigate these pressures, particularly through extended training periods for novice nurses and enhanced competencies for clinical educators, such as preceptors. Recent studies suggest that novice nurses require 8~12 months to fully understand and adapt to their roles [16, 17]. Additionally, preceptors often feel inadequately prepared and emphasize the necessity of structured guidelines for training novice nurses [18]. Internationally, training programs for new graduate nurses often exceed six months and include a range of methodologies, such as simulation-based residency programs, internships, and mentorships [19, 20]. In South Korea, pilot projects under the initiative to improve nurse shift systems have encouraged the establishment of dedicated education departments and institutionalized yearlong training programs for new graduate nurses [21]. Further research should evaluate the effectiveness of these policies and inform the development of structured education and training programs under the Nursing Act.
In large hospitals, professional identity was reinforced by the “Recognition and support for nursing professionalism” theme, reflecting a structured environment where nurses felt validated as critical members of the team. The alignment of roles, clear career pathways, and acknowledgment of contributions collectively enhanced their sense of professional worth. In contrast, nurses in small- and medium-sized hospitals described “Unstable professional iIdentity,” which was characterized by role ambiguity, insufficient resources, and a lack of professional recognition. Among the most prominent factors were “Unexpectedly poor working conditions” and “Unfair compensation,” which illuminated structural problems in the secondary labor market. Inequities in salary practices extended beyond low wages to include a lack of transparency, inconsistent criteria, and problematic payment systems, significantly affecting job satisfaction and stability [22]. Addressing these issues requires transparent salary systems, equitable wage policies, and fair compensation frameworks for overtime work.
The structural challenges in small hospitals are exacerbated by high turnover rates among temporary nurses awaiting permanent placement in large hospitals. This situation leads to a critical shortage of experienced personnel, disproportionately burdening newly qualified nurses. These novice nurses frequently find themselves handling complex, high-risk tasks without adequate preparation, further escalating their workload and stress levels. Moreover, the delegation of tasks traditionally performed by registered nurses to nursing assistants raises significant concerns regarding patient safety, ethical dilemmas, and role clarity. Compounding these issues is a shortage of physicians, which often forces nurses to make independent clinical decisions during night shifts or emergencies. This autonomy in critical situations increases their legal exposure and heightens stress, collectively fostering a high-pressure work environment that intensifies turnover intentions among nurses in small hospitals [23, 24]. These findings emphasize the structural disparities in workload contributors between large and small hospitals, underscoring the need for tailored interventions to address these distinct challenges.
One of the most pronounced structural issues highlighted in this study was the “Unstable professional identity” among nurses working in small- and medium-sized hospitals. This sharply contrasts with the “Recognition and support for nursing professionalism” category identified among nurses in large hospitals. Existing literature has shown that nurses often experience identity conflicts when they are viewed as mere task performers, encounter ambiguity in their roles, and endure inequitable treatment that undermines their professional standing [25, 26]. Participants in this study reported frequent role substitution, where nursing assistants assumed responsibilities typically assigned to registered nurses, while nurses were tasked with duties traditionally associated with physicians, such as proxy prescribing. These “Role Substitution and Ambiguity” scenarios fostered feelings of helplessness and diminished their sense of professional worth. In contrast, nurses in large hospitals felt validated as integral team members, reinforcing their professional identity. These findings underscore the importance of recognition, respect, and validation in bolstering professional identity, showing that economic incentives alone are insufficient for sustaining job satisfaction and retention.
Nursing identity is defined as the internalization of values, ethics, and behaviors associated with the nursing profession in relation to oneself and others. It encompasses domains such as values and ethics, knowledge, leadership, and professional comportment. Professional comportment refers to the expression of professionalism through attitudes, appearance, and behaviors and is realized through stable organizational structures [26]. Participants in this study noted that frequent changes in nursing management and vacancies in leadership positions undermined the role of the nursing division. Temporary hires and inadequate oversight of auxiliary personnel further contributed to the perception of instability within nursing organizational systems. Addressing these challenges requires not only improving physical and external factors, such as wages and benefits, but also reshaping managerial perceptions of nursing's significance. According to Grumbach et al. [27], monopsony and dual labor market structures in healthcare employment perpetuate chronic nursing shortages in small hospitals, as they struggle to compete with large hospitals in offering competitive wages. This exacerbates disparities between large and small hospitals. A comprehensive reassessment of supply-side solutions is necessary. Legislative and institutional efforts should prioritize establishing nursing-centered management systems to reinforce professional identity and address structural inequities in the nursing labor market.
This study identified structural differences in hospital selection and professional identity between large and small hospitals, reflecting the dual labor market characteristics of the nursing workforce. To address the imbalance in the supply and demand of nurses caused by this dual structure, efforts must go beyond merely increasing the number of nurses. Structural reforms are required to improve the working conditions of small hospitals and strengthen nurses' professional identity.
In South Korea, the recent enactment of the Nursing Act, long anticipated by the nursing profession, aims to strengthen nurses' rights and professional standing. However, specific legal measures to implement these goals must be detailed in enforcement decrees and regulations. Under the Nursing Act, tailored policies should focus on reducing workload intensity and fostering professional development opportunities in large hospitals to improve retention. In small hospitals, strengthening professional identity through structured mentoring programs, stable leadership, and clear role definitions is essential. Additionally, transparent salary systems and enforceable standards for auxiliary personnel oversight can address inequities and improve working conditions. Establishing nursing-centered management systems can further bridge disparities between large and small hospitals, ensuring equitable and sustainable workforce solutions.
The significance of this study lies in its exploration of the dual structure of the nursing labor market and its presentation of differences in hospital selection and professional identity between large and small hospitals. These findings contribute to diagnosing the imbalance in the nursing workforce and proposing solutions to address it. However, conducting FGIs in a virtual format increased accessibility for participants from diverse backgrounds but also introduced limitations, such as the potential impact of reduced non-verbal communication on data collection. Additionally, while some differences were observed between public and private hospitals, as well as among specialized hospitals like long-term care facilities, these were not the primary focus of this study and were therefore not extensively analyzed. Future research focusing on tailored strategies for workforce allocation based on the unique characteristics of small hospitals is recommended to address this gap.
Source of research fund or grant: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (Ministry of Science and ICT, MSIT) (No. RS-2024-00251515).