

Purpose
This study aimed to examine the validity and reliability of the Korean version of the Nurse-Nurse Collaboration Behavior Scale developed by Liao et al (K-NNCBS).
Methods: Data were collected through an online survey, of 258 nurses working in general or tertiary hospitals. We translated the NNCBS into Korean and evaluated it through content validity, criterion validity, reliability, and confirmatory factor analyses.
Results: The factor loading of the 23 items belonging to the four domains ranged from .40 to -.87. The confirmatory factor analysis supported a good model fit (χ2 =578.56, p<.001, CFI=.83, RMSEA=.08, SRMR=.07). Regarding criterion validity, the K-NNCBS was positively correlated with communication competence (r=.54) and negatively correlated with task conflict (r=-.22) and relationship conflict (r=-.29). Cronbach's ⍺ for K-NNCBS rated on a five-point Likert scale was .90.
Conclusion: These findings show that the K-NNCBS is valid and reliable. This scale can be used to measure the collaboration behaviors among nurses in Korea.
This study aimed to examine the validity and reliability of the Korean version of the Nurse-Nurse Collaboration Behavior Scale developed by Liao et al (K-NNCBS).
Data were collected through an online survey, of 258 nurses working in general or tertiary hospitals. We translated the NNCBS into Korean and evaluated it through content validity, criterion validity, reliability, and confirmatory factor analyses.
The factor loading of the 23 items belonging to the four domains ranged from .40 to -.87. The confirmatory factor analysis supported a good model fit (χ2=578.56, p<.001, CFI=.83, RMSEA=.08, SRMR=.07). Regarding criterion validity, the K-NNCBS was positively correlated with communication competence (r=.54) and negatively correlated with task conflict (r=-.22) and relationship conflict (r=-.29). Cronbach's α for K-NNCBS rated on a five-point Likert scale was .90.
These findings show that the K-NNCBS is valid and reliable. This scale can be used to measure the collaboration behaviors among nurses in Korea.
Interdisciplinary teams provide quality healthcare services to patients through their collaboration in various settings [1]. The shift to patient-centered care emphasizes the importance of interdisciplinary collaboration for provision of quality healthcare [2]. A failed collaboration or insufficient teamwork among healthcare professionals leads to medical errors. Such errors threaten patient safety, causing permanent injury or death [3]. Therefore, collaboration among healthcare professionals is a key requirement for patient care and its importance is rising gradually [4].
Interprofessional or intra-professional collaboration refers to team members sharing knowledge and resources for nurses to solve patient care or healthcare system problems [5]. Collaboration affects patients' interests and healthcare professionals' happiness and satisfaction [6]. Good collaboration and communication help nurses navigate stressful situations, support nursing practice, and balance work [7]. In constrast, poor collaboration causes turnover or dissatisfaction among medical professionals [8].
Nurses are key healthcare providers providing patient care around the clock and collaborating with each other during their shifts [9]. Such collaborative relationships help nurses realize their potential and competence [10]. As nurses form higher collaborations, their emotional intelligence and job satisfaction increases [8, 11], thus decreasing their turnover intention, and resulting in their provision of quality care to patients [12]. Close relationships and collaboration facilitate information sharing among nurses [13]. Contrarily, poor collaboration negatively affects patient outcomes, leaving patients dissatisfied with the treatment [14].
Previous studies have examined the degree of collaboration among nurses [11], nurses' perceptions of collaboration [15], and the relationship between nurses' collaboration and the incidence of medical errors [3]. Their findings highlight the importance of collaboration among nurses to ensure quality patient care and outcomes. Despite the importance of collaboration among nurses, studies have largely focused on the relationship between nurses and physicians [2, 3, 4, 8].
Instruments that measure collaboration among nurses include the Nurse-Nurse Collaboration (NNC) Scale developed by Dougherty and Larson [9]. The NNC Scale was developed based on the Intensive Care Unit Nurse-Physician Questionnaire, and focuses on communication and conflict management between nurses. However, since the questionnaire focuses solely on collaborative attitudes among nurses, collaboration among nurses can be confirmed, but the effect of this collaborative behavior on patient care cannot be measured. To complement these points, the Nurse-Nurse Collaboration Behavior Scale (NNCBS) was developed to measure cooperative behavior among nurses in the patient-centered treatment process [16]. The NNCBS consists of 23 questions in four subdomains: conflict management, common goal, communication and collaboration, and professionalism and autonomy. This scale also helps clinical nurse managers and educators intervene to enhance collaboration among nurses and examine the associations among nurses' behaviors, sociodemographic factors, and professional customary practice [16].
The "conflict management" subdomain of the NNCBS is an essential component of collaboration and promotes cooperation while suppressing hostility and uncooperative behavior among nurses. It enhances the ability to build and maintain interpersonal relationships and resolve conflicts. "Common goal" refers to mutual expectations of responsibilities and goals in patient care and involves discussions regarding differences in patient care planning and performance. "Communication and collaboration" refers to nurses' ability to complement and balance out each other and value equality. "Professionalism and autonomy" refers to behavior in which nurses claim professional expertise and professional opinions on patient treatment. Further, conflict resolution through negotitation is essential in creating a mutually acceptable resolution. Accordingly, the Global Interpersonal Communication Competency (GICC) scale [17] confirmed the validity of NNCBS by confirming its ability to facilitate comprehensive communication between professionals and nurses through relief from social tension, argumentation, interaction management, support, efficiency, social appropriateness, response, and noise control. In addition, the Intragroup Conflict Scale (ICS) [18] confirmed the presence of conflicts and relationship conflicts between nurses and quality patient care within the organizations.
The NNCBS helps nurses to collaborate and care for patients in a variety of ways, including ways to resolve disagreements, discuss and counsel for patient care, share patient information, and prepare and professionalize work for patient care. However, there is no Korean version of the NNCBS; thus, it cannot be widely used in Korean research. Therefore, we aimed to develop a Korean version of the NNCBS that reflects the clinical situation in Korea to keep pace with the transition to patient-centered treatment and evaluate its feasibility and reliability. The use of the K-NNCBS is expected to raise awareness of the cooperation required for patient care and contribute to basic data for necessary cooperation and program development.
In this methodological study, we translated the NNCBS developed by Liao et al.[16] into Korean, and evaluated the validity and reliability of the K-NNCBS.
As the NNCBS is a tool to measure collaboration among nurses in patient care, we selected nurses from general or tertiary hospitals with sufficient training. We excluded administrative nurses and chose only those nurses who collaborate with other nurses in patient care. Furthermore, nurses with less than six months of working experience were excluded from the study, based on the previous study [19] that it takes at least 10 to 180 days for new nurses to receive education and training after joining the company to independently perform patient care.
To validate a measure via factor analysis, at least 10 cases are needed per parameter [20]. Thus, data were collected from 260 nurses based on 23 items in the NNCBS and potential dropouts (10%).
Nurse-nurse collaboration behavior was measured by translating the NNCBS into Korean after obtaining approval from the original author Liao. The NNCBS comprises 23 items, with five items for conflict management, three items for common goals, seven items for communication and coordination, and eight items for professionalism and autonomy. Items are rated on a five-point Likert scale, ranging from never (1) to always (5), with higher scores indicating better nurse-nurse collaboration. The reliability of the original tool was .93, as measured with Cronbach's α, with the following values for each subdomain .86 for conflict management, .79 for common goals, .88 for communication and coordination, and .88 for professionalism and autonomy.
Participants' communication competence was measured using the Global Interpersonal Communication Competence (GICC) scale developed by Hur [17], after obtaining approval from the original author. This tool was developed in Korea, and comprises 15 items, with one item for each of the following: self-disclosure, empathy and perspective-taking, social relaxation, assertiveness, concentration, interaction management, expressiveness, supportiveness, immediacy, efficiency, social appropriateness, conversational coherence, goal detection, responsiveness, and noise control. The items are rated on a five-point Likert scale ranging from never (1) to always (5), with a higher score indicating better communication competence. Cronbach's α was .72 at the time of the tool development, and .77 in this study.
Intraorganizational conflict was measured using the Intragroup Conflict Scale (ICS), which was developed by Jehn [18] and translated into Korean by Song [21] after obtaining approval from the original author Jehn. This tool comprises eight items, with four items for task conflict and four items for relationship conflict. The items are rated on a five-point Likert scale ranging from strongly disagree (1) to strongly agree (5), with a higher score indicating a greater level of conflict. At the time of scale development, Cronbach's α was .87 for task conflict and .92 for relationship conflict, while in the study by Song [21], Cronbach's α was .81 and .82, respectively. In this study, Cronbach's α was .87 for task conflict and .85 for relationship conflict.
The translation and adaptation processes were performed according to the World Health Organization guidelines. We strived to ensure cross-cultural equivalence. The development process included translation, expert review, back translation, expert panel review, and finalization.
The English NNCBS was first translated into Korean by the researchers, considering the professional terminology used by Korean nurses. Researchers focused on conveying the meaning of a sentence rather than a literal word-to-word translation, while ensuring accuracy and conciseness. A preliminary draft was developed after discussion and consensus among the researchers. The draft was then reviewed by a professional translator to confirm its accuracy and the appropriateness of the expressions in the Korean context. The Korean translation draft was finalized with modifications after a review (K-1). The translated NNCBS (K-1) was then back translated by a bilingual professional (B) who had no prior knowledge of the original tool. The translator (A) and back translator (B) worked independently. The back translated version was compared with the original tool, and the second draft of the Korean version of the NNCBS (K-2) was developed, after considering cultural differences to convey an accurate meaning. To determine this version's clinical relevance, five clinical nurses along with a nursing professor, holding a minimum of bachelor's degree and nine 9 years of experience, reviewed the version. After modifying unclear or inappropriate items, the third draft of the preliminary Korean version of the NNCBS (K-3) was finalized.
Finally, the third draft (K-3) was reviewed by a Korean language major (C), for grammar and wording, to finalize the Korean version of the NNCBS (Appendix 1).
The content validity was evaluated by a panel of eight experts comprising two nursing professors, three hospital nurses with more than five years of experience, and three nursing PhDs with prior experience in scale development. The relevance of each item was rated on a four-point Likert scale (ranging from 4=highly relevant to 1=not relevant). Based on the responses, the item-content validity index (I-CVI) was calculated as the percentage of experts who gave 3 or 4, and scale-content validity index/average (S-CVI/Ave) was calculated by dividing I-CVI by the total number of items computed. Based on the study by Lynn [22], the cutoff for I-CVI to .78 or higher, and that for S-CVI/Ave was set to .90 or higher, to determine content validity. The S-CVI/Ave of the 23 items of the K-NNCBS was .95, and one item (item 12: The nurses share information with patients about the nursing protocol that is either ongoing or already done) had an I-CVI of below .78. However, item 12 was included because its I-CVI (.75) was close to the cutoff, and it was deemed necessary to measure communication and coordination.
Data from 260 nurses were collected from November 26 to December 2, 2020. After excluding two patients with incomplete responses, 258 nurses participated in the study.
The participants were recruited by posting recruitment advertisements on online nurse community bulletin boards (https://cafe.naver.com/angel2nurse) and social media, including Instagram, KakaoTalk, and Facebook. Volunteers who decided to participate were provided with the study information sheet and consent form.
This study was approved by the Institutional Review Board of Ewha University (IRB No. ewha-202011-0011-02). Participants provided informed electronic consent prior to beginning the questionnaire. The consent form specified the purpose, content, and confidentiality of the study, and participants could withdraw from the study at any time.
Data were analyzed using the SPSS 25.0 and AMOS 23.0 software. Participants' general characteristics were analyzed using descriptive statistics. The fit of the model was evaluated using the χ2 test, comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). The convergent validity of the items was evaluated using standardized estimates (β), construct reliability (CR), and critical ratio (C.R.). And their discriminant validity was evaluated using Pearson correlations among the factors of the K-NNCBS. Criterion validity was evaluated, through the correlation between and intraorganizational conflict, using Pearson correlation. The validity of the K-NNCBS increased with increasing positive correlation with the GICC, and a negative correlation with the ICS. The reliability of the K-NNCBS and its factors was assessed based on the internal consistency index, Cronbach's α.
Participants' average age was 28.2±4.9 years, and 244 (94.6%) were women. Most participants had a bachelor's degree (84.5%). The mean total clinical experience was 53.9±47.3 months, and the mean experience at the current unit was 32.5±27.0 months. Further, 51.9% of the participants wanted to work in their current unit, and many nurses (45.3%) worked in the general ward. The most common working type was an eight-hour rotating shift (91.1%), and the majority (87.6%) were staff nurses (Table 1).
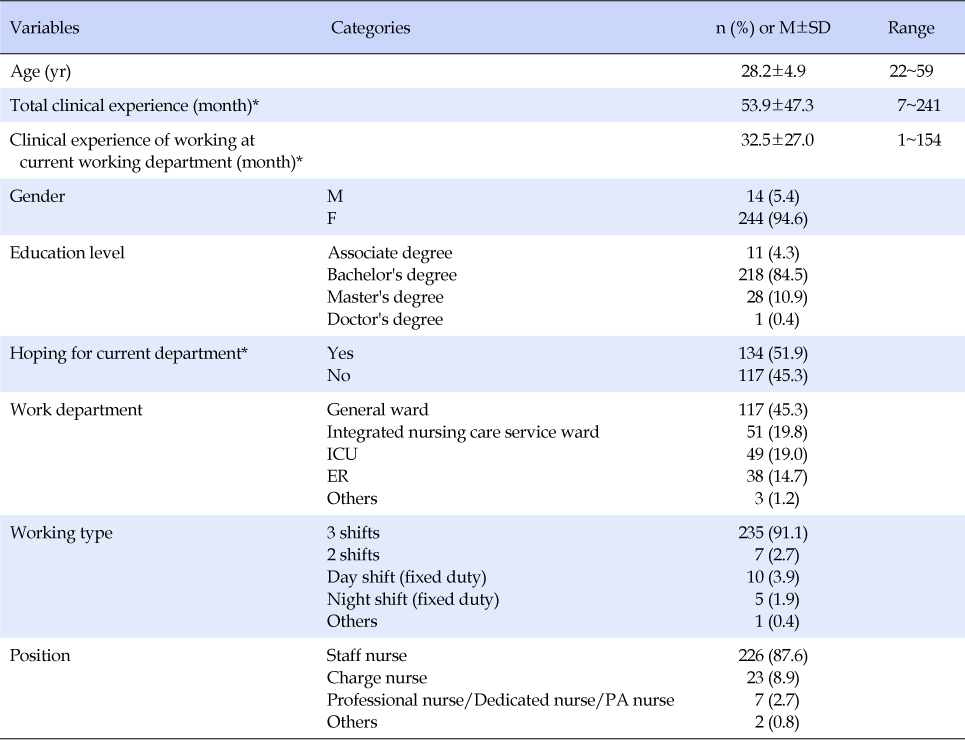
Table 1
Participants' General Characteristics (N=258)
The model fit of the K-NNCBS was analyzed using CFA for the four factors identified during scale development (Figure 1, Table 2). The results indicated a good model fit (Table 3). The CR was between .72 and .84, thus establishing the convergent validity (Figure 1, Table 2).
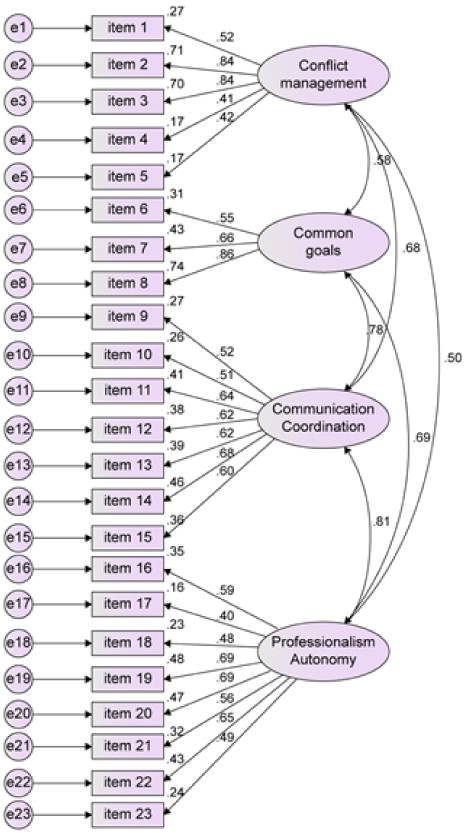
Figure 1
Confirmatory factor analysis of the Korean version of the Nurse-Nurse Collaboration Behavior Scale.
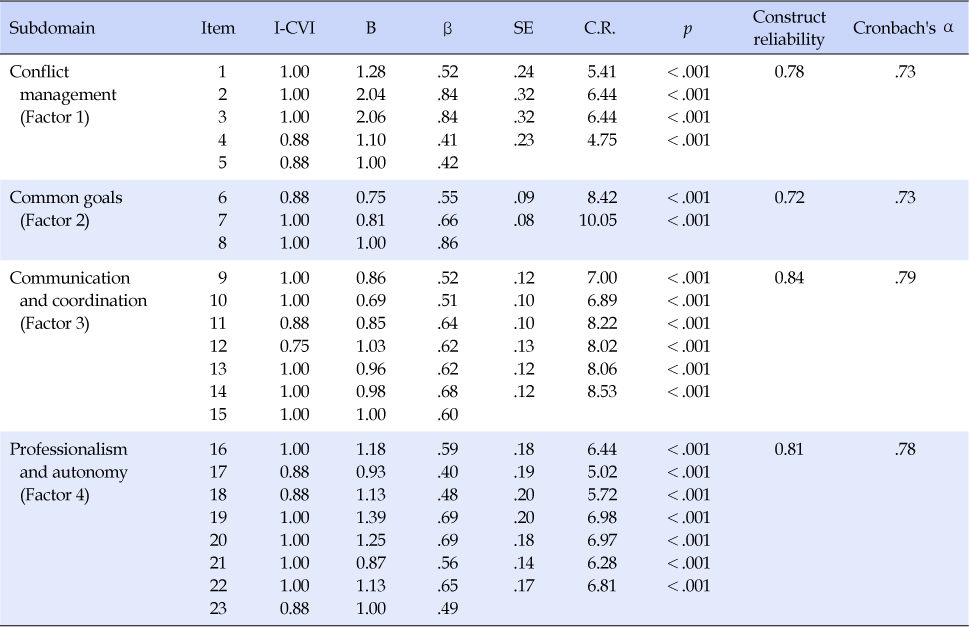
Table 2
Analysis of the Convergent Validity of Items (N=258)

Table 3
Model Fit Indices of the Korean Version of the NNCBS (N=258)
The correlation coefficients between the K-NNCBS factors were lower than .90, as recommended by Kline [20], establishing the discriminant validity (Table 4).
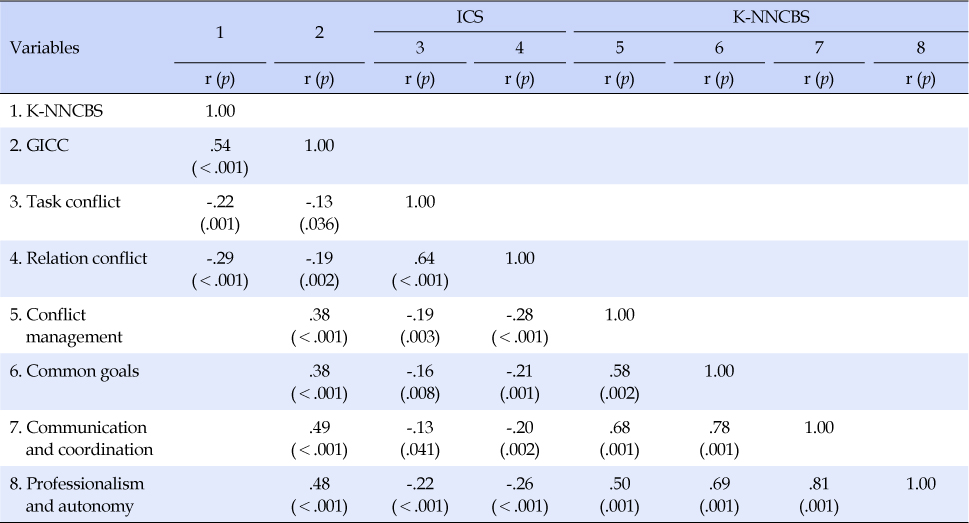
Table 4
Discriminant and Criterion Validity of the Korean Version of the K-NNCBS (N=258)
Criterion validity was evaluated by analyzing the correlation of the K-NNCBS with GICC, task conflict, and relationship conflict of the ICS. The 23 items of K-NNCBS had a significant positive correlation with GICC (r=.54, p<.01) and a significant negative correlation with task conflict (r=-.22, p<.01) and relationship conflict (r=-.29, p<.01), confirming the criterion validity of the scale (Table 4). The four factors had a significantly positive relationship with GICC and a significantly negative relationship with task conflict and relationship conflict of the ICS (Table 4).
Cronbach's α was .90 for the overall scale, .73 for conflict management, .73 for common goals, .79 for communication and coordination, and .78 for professionalism and autonomy (Table 2).
This study aimed to translate the NNCBS and validate its Korean version. The validity and reliability of the K-NNCBS were evaluated with evidence based on content validity, construct validity, and criterion validity.
The K-NNCBS had an S-CVI/Ave of .95 and I-CVI of 0.75~1.00, where all but one item met the cutoff of .78; thus, the instrument had valid content for measuring nurse-nurse collaboration. Item 12, "The nurses share information with patients about the nursing protocol that is either ongoing or already done." had an I-CVI of .75. This item may have received a low relevance rating as the K-NNCBS measures nurse-nurse collaboration while this item pertains to sharing information with patients. In addition, there may still be a lack of awareness among nurses in Korea that collaboration behavior has a direct effect on patient-centered nursing. However, we included the item in the scale because nurse-patient information sharing involves patients in their treatment-related decision-making, reduces nurses' uncertainty, and helps them make better decisions [24], which are necessary for measuring nurses' collaboration.
The NNCBS was developed through a theoretical framework and validated with its four factors (conflict management, common goal, communication and coordination, and professionalism and autonomy). As CFA is appropriate for validating the translation of a previously validated scale [25], we performed CFA on a model comprising four factors used in the original tool, for validity testing based on internal evidence. As the χ2 test for evaluating model fit is heavily influenced by sample size, it is necessary to select both relative and absolute fit indices to test the model fit [26]. Thus, χ2/df, CFI, RMSEA, and SRMR were chosen for model fit evaluation. The criteria for a good model fit are χ2/df≤3, CFI≥.90, SRMR≤.08, and RMSEA≤.08, as proposed by Kline [20]. The K-NNCBS had an χ2/df of 2.58, CFI of .83, SRMR of .07, and RMSEA of .08. Although not all criteria were met, it was considered a relatively good model, retaining the four-factor structure of the original tool. The standardized estimates (β) were .40 or higher for all items. Items 4, 5, 17, 18, and 23 showed relatively low β values. Item 4, "All nurses try to avoid conflict," and Item 5, "Any conflicts or disagreements among nurses are resolved quickly and peacefully," are about conflicts between nurses, not about nurses' caring behavior in collaboration with other nurses. Participants considered them to be independent of nurses' caring behavior, and the measured value was thus low. However, these items were not deleted because conflicts between nurses can lead to strained relationships, which affect nurses' caring behavior. Item 18, "I have input regarding my desired shift," might have a low β because it does not directly affect nurses' caring behavior as items 4 and 5 do. However, nurses who care for inpatients work in shifts to care for patients 24 hours a day, and there is a limit to adjusting the desired schedule without consideration of or collaboration with other nurses; therefore, it is suitable for this scale. Item 17, "Nurses avoid the use of procedures that violate aseptic principles" (β=.40), and item 23, "Nurses avoid the use of procedures that compromise patient safety" (β=.49) had low β values. While other items focused on the degree of collaborative behavior, these two items emphasized the avoidance of behaviors that hinder professionalism, which is a sub-construct of collaborative behaviors. There may be insufficient explanation regarding the professionalism of nurses in the Korean clinical situation. The construct reliability value was between .72~.84, confirming convergent validity, and the correlation coefficients for the items were .90 or lower, confirming discriminant validity. Hence, construct reliability of the 23-item K-NNCBS was established. However, there is a limit to comparing and analyzing the results of this study, because at the time of developing the original tool, previous studies had only measured the validity of the NNCBS. Therefore, to utilize the K-NNCBS tool in Korea, repeated studies on its validity are required for nurses working in various clinical environments.
Criterion validity refers to the correlation between the newly developed tool to measure the studied concept and the gold standard in the field. Currently, the tool used to measure collaboration among nurses in Korea is a translation of an overseas tool; its reliability and validity have not been evaluated. Therefore, it was difficult to select the gold standard for this study. Accordingly, we evaluated the criterion validity through communication competence and conflict, which are crucial elements in this subdomain. GICC and ICS measured the concepts, within a general organization. However, K-NNCBS measured the concept of nurses providing patient care in hospital setting. Regarding the criterion validity, there was a significantly positive correlation between the K-NNCBS and GICC scores, showing that nurses' collaboration behaviors increased with the increase in communication competence. This is similar to previous findings showing that communication helps foster relationships among healthcare providers [27]. There were significantly negative correlations between the K-NNCBS and task conflict and relationship conflict scores, where nurses' collaboration behaviors decreased with increasing task and relationship conflicts. This is consistent with previous findings in which coherence decreased with increasing relationship and task conflicts [28]. These results thus established the criterion validity of the K-NNCBS.
Regarding the reliability of the K-NNCBS, Cronbach's α for the overall scale was .90, which was similar to the original Cronbach's α of .93, confirming its reliability. Cronbach's α for each factor ranged from .73 to .79. These were slightly lower than the values for the original scale, but the common goal factor had a value higher than .70 even with three items. Further, based on the criteria suggesting Cronbach's α of .70, as adequate, .80 as good, and.90 as excellent [29], no problems would arise with factor-specific analysis.
Collaboration is an important part of nursing competency and is directly related to patient safety, ; For example, it helps in providing high-quality patient care and reducing medical errors [9]. Recently, the number of comprehensive nursing care service wards has increased [30]. The nurses working in comprehensive nursing care service wards provide inpatient nursing care in collaboration with other nurses without a caregiver, leading to an increase in [30]. The direct nursing time and the importance of the role of collaboration among them Therefore, the K-NNCBS may be useful for developing programs that promote collaboration in Korea. Ultimately, it is meaningful as it can reduce medical errors caused by communication and coordination problems through collaboration between nurses and improve patient outcomes by providing high-quality patient care.
This study validated the K-NNCBS for the first time in Korea, establishing it as an appropriate instrument for measuring collaboration among Korean hospital nurses. However, we only conducted a CFA for the K-NNCBS. Subsequent studies should conduct an exploratory factor analysis to generate varying factor structures, depending on the other country and participants. Nurse-nurse collaboration is influenced by variables such as individual characteristics, leadership, and job satisfaction; therefore, further studies should focus on more diverse nurses are needed. Continued follow-up studies would further enhance the reliability and validity of the scale and enable comparisons among nurses in various work settings.
This study translated and validated the NNCBS into Korean, in consideration of Korea's clinical setting. This study established the reliability and validity of the tool based on content validity, construct validity, and criterion validity. Collaboration between nurses affects both patients and nurses. The K-NNCBS can help measure the collaboration of nurses in the Korean clinical setting and find appropriate solutions by finding out which domain are problematic when collaboration is difficult.
