

Purpose
This study investigated the mediating effect of patient participation culture in the relationship between ethical leadership and performance in patient-engaged nursing services.
Methods
This study employed a cross-sectional descriptive online survey design. The sample comprised 104 nurses from small- and middle-sized Korean hospitals.
Data were collected between May 10 and September 10, 2019 using the Smart Patient Engagement Assessment Checklist, Korean versions of the Patient Participation Culture Tool for healthcare workers, the Ethical Leadership Scale, and a questionnaire about nurses' demographic and work characteristics. A mediation analysis was conducted using multiple regression and a simple model applying the PROCESS macro using SPSS/WINdows software version 26.0.
Results
Ethical leadership directly affected (c'=0.28, p<.001) performance in patient-engaged nursing services. Patient participation culture partially mediated the relationship between ethical leadership and performance in patient-engaged nursing services (a ․ b=0.51×0.20=0.10, 95% Boot CI=0.18~0.20).
Conclusion
Optimizing the patient participation culture and adherence to ethical leadership among hospital administrators and managers can improve nurses' performance in patient-engaged nursing services. Nurse managers' ethical leadership should be strengthened, and patient participation culture should be encouraged at policy levels through systematic nurse education on patient safety and engagement to enhance performance-engaged nursing services.
This study investigated the mediating effect of patient participation culture in the relationship between ethical leadership and performance in patient-engaged nursing services.
This study employed a cross-sectional descriptive online survey design. The sample comprised 104 nurses from small- and middle-sized Korean hospitals. Data were collected between May 10 and September 10, 2019 using the Smart Patient Engagement Assessment Checklist, Korean versions of the Patient Participation Culture Tool for healthcare workers, the Ethical Leadership Scale, and a questionnaire about nurses' demographic and work characteristics. A mediation analysis was conducted using multiple regression and a simple model applying the PROCESS macro using SPSS/WINdows software version 26.0.
Ethical leadership directly affected (c'=0.28, p<.001) performance in patient-engaged nursing services. Patient participation culture partially mediated the relationship between ethical leadership and performance in patient-engaged nursing services (a · b=0.51×0.20=0.10, 95% Boot CI=0.18~0.20).
Optimizing the patient participation culture and adherence to ethical leadership among hospital administrators and managers can improve nurses' performance in patient-engaged nursing services. Nurse managers' ethical leadership should be strengthened, and patient participation culture should be encouraged at policy levels through systematic nurse education on patient safety and engagement to enhance performance-engaged nursing services.
Patient engagement improves health outcomes by improving patient safety and encouraging active involvement of patients and their families is a prerequisite for healthcare institutions [1]. Patient engagement is essential for providing patient-centered and safe healthcare services [1]. Direct outcomes, like decreasing sentinel events and length of stay and increasing financial profit, have been reported in healthcare services [2]. Increasing patient engagement involves diverse factors related to patients, health professionals, and organizations [3]. According to the interactive care model [4], facilitating a process that enables healthcare providers to engage patients more proactively in providing their care can lead to the effective tailoring of interventions and improved care quality, safety, and outcomes at lower costs. With the pros of patient engagement, hospitals have tried providing patient-engaged services in nursing, like bedside handoff [5] and the nurse in charge of education [6]. However, the nurses perceived the patient-engaged nursing services as a burden due to a lack of resources and time for training to adapt to the new service system [7]. Therefore, to foster patient engagement, at an organizational level, nursing managers and administrators need to form an organizational culture so that patient engagement is not recognized as a hindrance to nursing work but as an essential factor for promoting patient safety and health [8].
Ethical leadership in nursing where a high degree of work ethic is emphasized is the need of the hour [9]. In the clinical field, many niches of nursing require making high-level ethical decisions while caring for patients. Still, because there are no clear guidelines, they are influenced by nursing managers who clearly understand the value and vision of the organization and have competency for ethical value judgement [10]. Ethical leadership is "a leader setting an example of normatively appropriate behavior through his or her own behavior and interpersonal relationships and promoting members to act ethically appropriately through two-way communication, reinforcement, and decision-making." [11] In other words, leaders' ethical leadership is a concept learned and strengthened by members during interaction between leaders and members. Leaders should not only set an example of ethical behavior but also set ethical standards and enhance them using rewards and regulations [12]. Previous studies have shown that ethical leadership directly impacts organizational performance, like nursing performance [13], organizational commitment, work engagement, organizational citizenship behavior, job satisfaction, and turnover intention [14]. Despite the importance of the relationship between ethical leadership and nursing outcome, to our knowledge no study has thus far examined the effect of ethical leadership on patient-engaged nursing performance.
For small- and middle-sized hospitals, with poor working environments and staffing, active use of patient engagement strategies is particularly beneficial for improving patient safety [15]. As of 2016, Korea's small- and middle-sized hospitals had a patient-to-nurse ratio of 24:8, twice that of general tertiary hospitals [16]. Furthermore, it was reported that the medical staff at smaller hospitals showed lower sensitivity toward patient safety [17]. Studies found that patient mortality is lowered when the number of patients per nurse is low [18], which leads to fewer medication errors and sentinel events [19]. It is difficult for nurses in small- and middle-sized hospitals to pay attention to patient safety because of the poor working environment and shortage of human resources. According to Lee et al.[20], the performances of patient-engaged nursing services of nurses working in hospitals with more than 1,000 beds is significantly higher than those working in hospitals with more than 500 beds and less than 1,000 beds. This is because the organizational resources and environment difference, where systems and procedures are supported in a relatively stable manner, affected nurses' performance [20]. Therefore, it is necessary to identify the influencing factors on the performance of patient-engaged nursing services by nurses exposed to poorer working environments in small and medium-sized hospitals.
Culture represents patterns of values, beliefs, and retained ways of coping with experiences that develop over an organization's history. It tends to manifest in its members' material structures and behaviors [21]. Like most interactive behaviors, the behaviors of healthcare workers are inherent in group culture. Patient participation culture refers to all combinations of personal and organizational factors and behaviors that relate to how things work around, thus, regarding sharing power and responsibility for patient participation [22]. The World Health Organization [23] announced that creating a culture of patient participation for patient safety facilitates patient-provider relationship so that families and patients can access sufficient health information and understand the healthcare process accurately. Effective leadership and supportive culture are vital for enhancing patient safety in primary care. This suggests building an environment where professionals and patients can speak up about health and safety issues that they are concerned about without any hesitation [23]. Although an association between the performances in patient-engaged nursing service and patient participation culture has not been established, patient participation culture positively affecting health outcomes is widely recognized . According to Barello et al. [24], patient participation climate affects health literacy through the patient health engagement model. This indicates, healthcare systems can execute a new paradigm where patients play an independent role in their healthcare.
Nurses play a critical role in helping patients actively engage in their own healthcare. Through the relational and educational aspects of nursing care, nurses can support patient engagement, which improves patients' quality of life [25]. In addition to the individual efforts of nurses, positive results can be achieved only when managers' and organizations' support are combined. However, patient engagement research is in its infancy in Korea, and no study till date has examined the relationship between nurses' performance in patient-engaged nursing services, managers' leadership, and patient participation organizational culture.
Therefore, in this study, we aimed to explore relationships between the ethical leadership of nurse managers, the culture of patient participation, the level of performance in patient-engaged nursing services perceived by nurses in small and medium-sized hospitals, and to verify the mediating effect of the culture of patient participation in the relationship between the ethical leadership of managers and the performance in patient-engaged nursing services. Therefore, it is intended to provide fundamental data for improving the quality of nursing services and patient safety.
This study employed a cross-sectional design to investigate the mediating effect of patient participation culture in the relationship between ethical leadership and performance in patient-engaged nursing services.
The research participants are staff or charge nurses who perform direct nursing care to patients at small- and medium-sized hospitals (50~299 beds) in Korea, who understand the purpose and method of this study and agree to participate in the study. Also, participants were selected using the stage of clinical competence [26]. To consider the orientation period for working independently in the working department [27], nurses who worked over six months were eligible to participate. A total of 142 nurses, the sample size was calculated using G*Power 3.1.7 for Windows (effect size=.15; α error probability=.05; power=.80; number of predictors=10) considering the 20% dropout rate, working in small- and medium-sized Korean hospitals (50~299 beds) were recruited via an online self-report questionnaire that took 20~25 minutes. Data of 38 participants were excluded due to incomplete responses or the inclusion criteria not being met, and our final sample thus comprised 104 participants. In this study, data from 104 people were collected and analyzed, and the power of the collected data was 0.89.
Participants were recruited through convenience sampling, using a list of medical institutions uploaded on the Korean National Health Insurance Review & Assessment Service website. Researchers explained the study's purpose and requested cooperation by phone to 43 hospitals' nursing department of the 126 hospitals with more than 50 beds and less than 300 beds in the list; from 38 responded and requested detail research information excluding 5 hospitals that refused to participate in the study. Participants were recruited by posting a recruitment notice, with the online survey link, on the online and offline bulletin boards of the nine hospitals that accepted research cooperation after reviewing the research proposal. Data was collected from May 10 to September 10, 2019.
The dependent variable was performance in patient-engaged nursing services. The independent variables were ethical leadership and patient participation culture.
The covariates included demographic characteristics-gender, age, and education-and work characteristics-number of hospital beds, work experience, current position, current working unit, nursing delivery system, patient safety education experience, and patient engagement awareness. Patient engagement awareness was measured using the yes/no question.
Performance in patient-engaged nursing services was assessed using the Smart Patient Engagement Assessment Checklist [20]. This tool was developed based on the contents presented as an inspection item that hospitals should perform to promote patient engagement in accordance with the Guide to Patient and Family Engagement in Hospital Quality and Safety of the Agency for Healthcare Research and Quality (AHRQ) [25]. At the time of development, 37 questions in four areas ((a) working with patient and families as advisors (8 items), (b) communication to improving quality (6 items), (c) bedside patient handoff (10 items), (d) discharge planning (13 items)) after a review by two nursing university professor and two nurses with 20 years of clinical experience, and the response to each question consisted of three things; ‘implementation’, ‘unimplemented but clinical application is required’, and ‘unimplemented and clinical application is not required’ to identify implementation status and necessity of application. In this study, with the permission of tool developers some questions were excluded and each item rated 1 (Yes, I perform it) or 0 (No, I do not perform it). The deleted questions were excluded because there was a possibility of over-estimation of certain parts, with 9 items of bedside patient handoff, which cannot be answered without performing bedside patient handoff, and one question of communication that can be answered in duplication in the original tool. It includes 27 items across four sub-scales ((a) working with patients and families as advisers (8 items), (b) communicating to improve quality (5 items), (c) bedside patient handoff (1 items), and (d) discharge planning (13 items); total 0~27; a higher total score represents better performance in patient engagement nursing services). This instrument was not tested for reliability when it was developed; however, in this study, KR20=.93.
The Korean version of the Ethical Leadership Scale [11, 28], modified to fit the hospital context, was used to assess the ethical leadership of nursing managers as perceived by nurses. In order to increase the clarity of meaning when translating from English to Korean, the subject‘my boss’ was added [34], and in this study, it was revised to ‘my boss (nursing manager) to fit the hospital context. This instrument includes 10 items rated on a five-point Likert scale (1=Strongly Disagree to 5=Strongly Agree; total 5~50). The higher the total score, the more nurses perceive their leaders as ethical. The measure has high reliability: Cronbach's α=.96 in the current study, .91 in the original study, and .91 in the translated version.
The organization's culture of patient participation was measured using the Korean version of the Patient Participation Culture Tool for healthcare workers [22], translated by Shin [29] and modified through translation and backtranslation by Korean-English bilingual healthcare professionals from the current study. The existing translation directly translated the sentence "patient partnership leads to short term loss of time in the individualized care of the patient", however, in this study 'individualized management for patient participation requires a lot of time in a short period of time.' revised to Korean that can be understood and read more smoothly. It comprises 52 items across eight sub-scales: (a) competence (3 items), (b) support (8 items), (c) perceived lack of time (3 items), (d) information sharing, and dialog (18 items), (e) type of question: factual questions (5 items), (f) type of question: challenging questions (4 items), (g) type of question: notifying questions (4 items), (h) acceptance of a new role (7 items). All items are rated on a four-point Likert scale (1=Fully disagree, 4=Fully agree; total 52~208); a higher score indicates better patient participation culture. This instrument has a high level of reliability: Cronbach's α=.94 in this study, .92 in the development study, and .89 for the translated version.
The collected data were analyzed using SPSS 25.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics such as the mean, standard deviation (SD), and proportions were used to present sample characteristics. The t-test and one-way analysis of variance were used to compare performance in patient-engaged nursing services, patient participation culture, and ethical leadership, among general and work characteristics. Pearson's correlation coefficient was used to analyze the relationships among major variables, and factors associated with performance in patient-engaged nursing services were analyzed using multiple linear regression using Baron and Kenny's three-step mediating effect test [30]. The statistical significance of the mediating effect was tested by Sobel test. Before testing mediating effect, the multicollinearity (VIF) between independent variables and the self-correlation of dependent variables (Durbin-Watson) were confirmed, and Kolmogorov-Smirnov's analysis and Breuch-Pagan test and Koenker test were conducted for the suitability test of regression model. The Durbin-Watson index was calculated using the EasyFlow Statistical macro [31]. Variables with a p value of <.1 in univariate analyses were retained in the final regression model. Statistical significance was determined by a p value of <.05.
This study was approved by the Institutional Review Board of Yonsei University Medical Center (Approval No: Y-2019-0029). This study used an online survey so that staff nurse can honestly respond to the leadership of their managers. All participants received information about the study on the first page of the online survey link, which guaranteed their confidentiality and underlined that their participation was voluntary and could be terminated at any time. After securing anonymity by giving individual identification codes, the collected data was stored on a computer with limited access and lock settings, and a small gift was provided to the participants.
The demographic and work characteristics of the participants are presented in Table 1. Most participants were women (n=98, 94.2%), aged between 30 and 39 (n=42, 40.4%), and had a bachelor's degree or above (n=63, 60.6%). Approximately 67.3% of participants worked in hospitals containing between 200 and 300 beds. Most staff nurses (n=89, 85.6%) working in comprehensive nursing care service wards (n=40, 38.5%). More than half (n=53, 51.0%) had worked for longer than five years. Nearly half perceived their current unit's nursing delivery system as functional (n=49, 47.1%), 86.5% had received patient safety education in the past year, and 50% were aware of patient engagement.
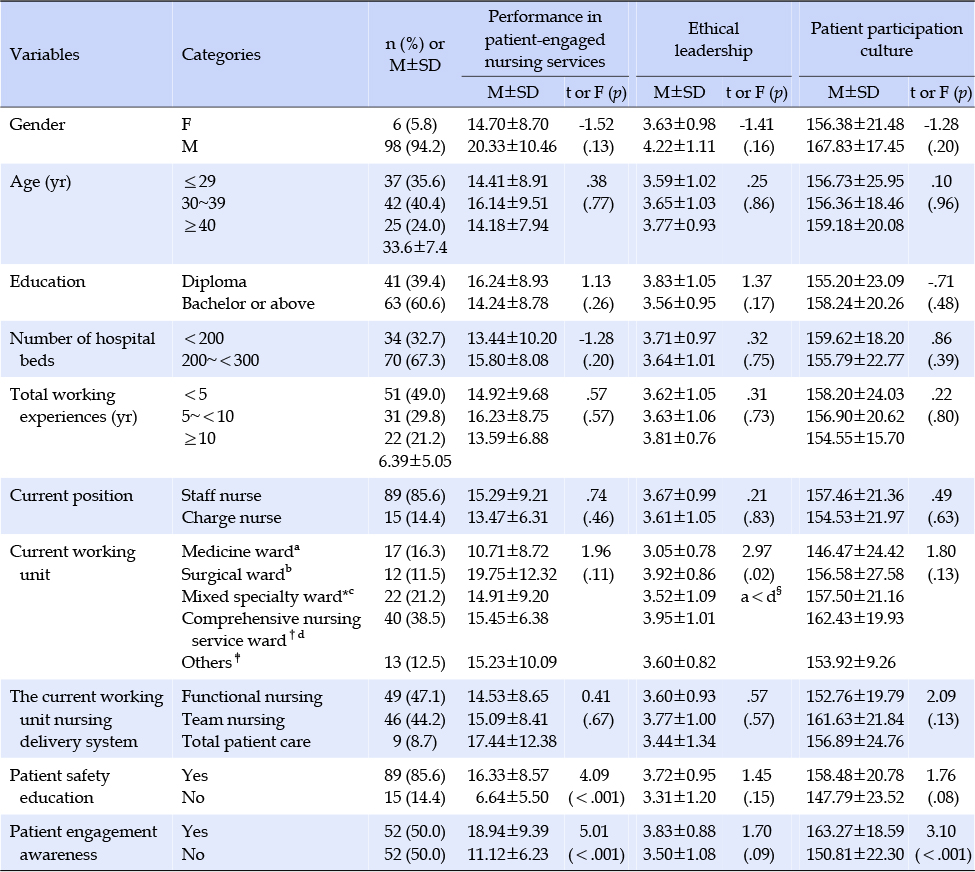
Table 1
Differences in Variables Based on General Characteristics (N=104)
The descriptive statistics on research variables are shown in Table 2. The average score of performance in patient-engaged nursing services was 13.59±7.15 out of 27 points. The average score for ethical leadership was 3.66±0.99 out of 5 points, and the average score for patient participation culture was 156.28±21.49 out of 208 points.
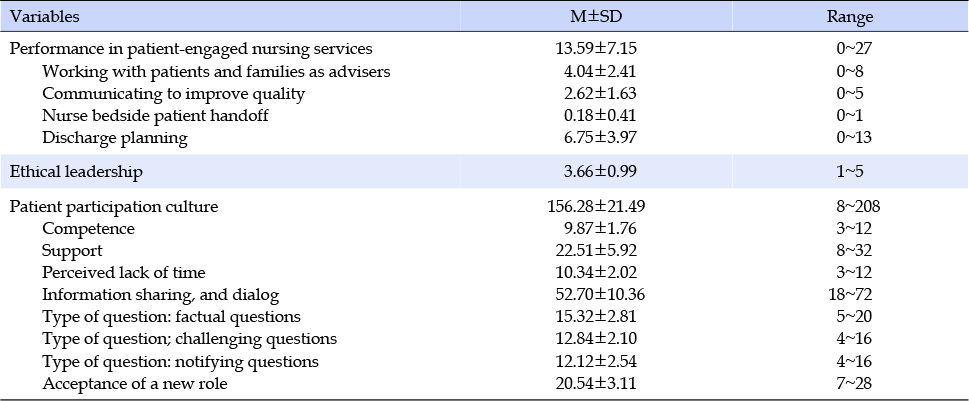
Table 2
Level of Performance in Patient-Engaged Nursing Services, Ethical Leadership, and Patient Participation Culture
As indicated in Table 1, in the group that completed patient safety education within the first year, the sum of performance in patient~engaged nursing services scores was higher on average than those who did not complete it (t=4.09, p<.001). The group had awareness on patient engagement scored higher in the performance of nursing services for patient engagement than the others (t=5.01, p<.001). Among participants' demographic and working characteristics, the factor showing a statistically significant difference in ethical leadership was ward type. In the differences in average ethical leadership score by current working unit by Scheffé post hoc test, the among nurses in the comprehensive nursing care service ward was higher than in the medicine ward (p=.04). The patient participation culture scores showed a significant difference depending on whether the participants had experience about patient engagement awareness. In other words, participants who had received education on patient engagement scored higher in patient engagement culture compared to those who never had the patient engagement education experience (t=3.10, p<.001).
Table 3 shows the correlations among variables. Performance in patient-engaged nursing services was positively correlated with ethical leadership (r=.48, p<.001). In the relationship between subscales of patient participation culture and performance in patient-engaged nursing services, competence (r=.31, p<.001), support (r=.56, p<.001), and information sharing and dialog (r=.46, p<.001) were significant positive correlation with performance in patient-engaged nursing services. In the relationship between ethical leadership and subscales of patient participation culture, competence (r=.43, p<.001), support (r=.64, p<.001), information sharing and dialog (r=.44, p<.001), type of question: factual questions (r=.23, p=.018), challenging questions (r=.26, p<.001), and acceptance of a new role (r=.30, p<.001) was positively correlated with patient participation culture.
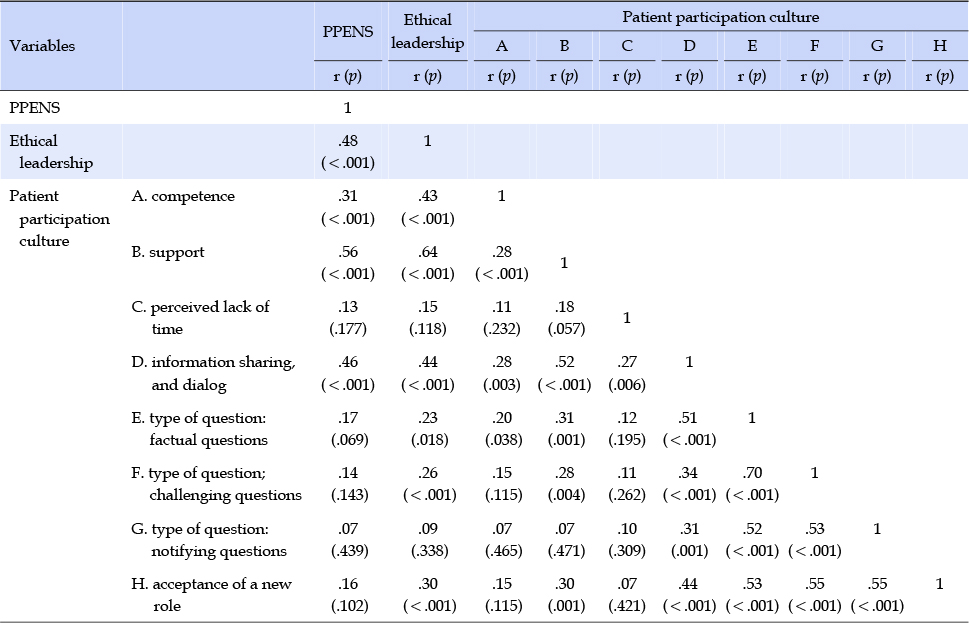
Table 3
Correlations among Performance in Patient-Engaged Nursing Services, Ethical Leadership, and Patient Participation Culture
The results of the mediating effects of patient participation culture on ethical leadership and performance in patient-engaged nursing services are shown in Table 4. In this study, the three-step method [32] conducted to analyze the mediating effect. In the first step, we analyzed the effect of ethical leadership on patient participation culture as a mediating variable. This confirmed that ethical leadership significantly affected patient participation culture (β=.51, p<.001). In step two, we analyzed the effect of ethical leadership on performance in patient-engaged nursing services as a dependent variable. As a result, ethical leadership had a significant effect on performance in patient-engaged nursing services (β=.39, p<.001). In the third step, patient participation culture, a parameter, was added and input as an independent variable along with ethical leadership, and performance in patient-engaged nursing services was added as a dependent variable. As a result, ethical leadership had a statistically significant effect on performance in patient-engaged nursing services (β=.28, p=.002), and also patient participation culture had a significant effect on performance in patient-engaged nursing services (β=.20, p=.028). These results suggest that ethical leadership and performance in patient-engaged nursing services are partially mediated by patient participation culture. Ethical leadership explained 41.0% of the variance in performance in patient-engaged nursing services, and the model including ethical leadership and patient participation culture explained 44.0% of the variance in performance in patient-engaged nursing services.

Table 4
Mediating Effects of Patient Participation Culture on Ethical Leadership and Performance in Patient-Engaged Nursing Services
In this study, the results of applying model 4 of the SPSS PROCESS macro [32] to test the mediating effect of patient participation culture in the relationship between ethical leadership and performance in patient-engaged nursing services. In addition, bootstrapping was performed, and the lower and upper limits of the indirect effect coefficient were analyzed in the 95% confidence interval. The analysis showed that the indirect effect was 0.10, which was strong enough to account for 39.0% of the total effect. As a result of the mediating effect test, patient participation culture between ethical leadership and performance in patient-engaged nursing services did not include zero between the lower limit value (0.18) and the upper limit value (0.20) of the confidence level (Figure 1). Therefore, this was statistically significant.
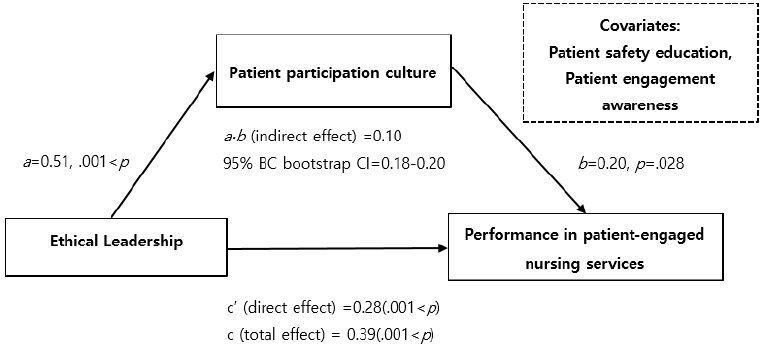
Figure 1
Statistical relationships for simple mediation model among ethical leadership, patient participation culture, and performance in patient-engaged nursing services while controlling for general characteristic variables.
In this study, we analyzed the associations of patient participation culture and ethical leadership with nursing services that facilitate patient engagement in middle-sized hospitals in South Korea, formulating strategies to improve their performance in patient-engaged nursing services. As a result of this study, the partial mediating effect of patient participation culture was confirmed as ethical leadership influences performance in patient-engaged nursing services.
First, this study identifies the level of ethical leadership, patient participation culture, and patient-engaged nursing service performance. The average level of ethical leadership for nursing managers was 3.66±0.99, higher than in studies of other occupational groups [28]. It is also higher than that of at four general hospitals in South Korea [33]. The higher score for ethical leadership stems from the recent emphasis on the value of ethical treatment in the hospital environment [34]. According to the Social Learning Theory, subordinates replicate the behavior of leaders who demonstrate normative and reliable behaviors [33], and ethical leadership of nursing managers affects nurses' ethical decision-making [35]. It can be thus understood that current managers learned and developed because of their managers' ethical leadership. This study found that nurses working in the comprehensive nursing service ward perceived the ethical leadership of nursing managers more than those working in general wards. This was somewhat different from the results of previous studies that showed differences according to marital status, and academic background of master's degree [13]. Furthermore, in previous studies, nurses working in specialized units like intensive care units and operating rooms had higher ethical leadership scores than those working in general wards; but in this study, it was noted that nurses in comprehensive nursing service ward had higher ethical leadership scores. This can be inferred that the supportive attitude and support of nursing managers was reflected through previous studies in which nursing managers' ability, leadership, and support scores for nurses were higher than those of general ward nurses [36].
Subcategories of patient participation culture can help understand obstacles and directions for improving performance. When comparing the subdomains, nurses scored 52.70±10.93 points for information-sharing and 21.30±3.07 for new role recognition in this study. These scores are higher than 48.76±10.74 and 18.98±3.02 scored in the study on 1,329 Belgian medical personnel using the same tool [22]. However, nurses' scores on attitudes to questions (factual, challenging, and informative) were generally lower in this study than above-mentioned Belgian study [22]. The lower score can be interpreted as reflecting the cultural characteristics of expressing respect for authority and encouraging silence to avoid confrontation [37]. Unlike our study, where there were no differences in performance in patient-engaged nursing services and patient participation culture according to age or career period, the Belgian study reported that older nurses were more inclined toward challenges associated with accepting new collaborative patient roles and coping with more active patients [38]. The Belgian study disclosed that sharing authority and responsibility, vital to promoting patient participation, can be considered as advanced skills that require specialized learning [38]. In our study, most of the nursing workforce was composed of unskilled nurses aged 20~29 years, which might explain the insignificant differences by experience. Therefore, it is possible to apply strategies to promote patient engagement through developing an undergraduate or on-the-job educational program, which is suggested by our research findings, to other countries with a similar workforce. Prior studies confirmed a statistically significant difference in the mean scores of perceptions of a "lack of time" (p=.02) between nursing managers and nursing staff [38]. Considering this disparity, together with the fact that most nurses already experience high labor pressure due to inadequate staffing [18], patient safety or patient engagement presented in a top-down manner is simply a new task that decreases patient engagement [38]. Emphasizing patient engagement without improving systemic efficiency and working environment may lead to an increase in nurses' turnover intention [39] and the omission of other necessary nursing care [40].
According to our knowledge, this study is the first to identify the degree of performance in patient-engaged nursing services despite there being a study that measures patients' level of patient engagement [41] or clinicians' attitudes or competencies related to patient participation [42]. The measurement used in this study are used for the first time in the domestic nursing field by scoring tool developed to record the responses with 'yes or no' to grasp the actual situation; there is a limit to direct comparison with other studies. As a result of this study, performance in patient-engaged nursing services was moderate at 13.59±7.15 out of 27 points. Among the general characteristics, there were significant differences in the group that completed patient safety education within the first year and in patient engagement awareness. Many South Korean nursing colleges have recently launched patient safety classes [43], which requires that the World Health Organization guidelines [44] for patient engagement to be included. The effect of the change in the curriculum on performance in patient-engaged nursing services must be studied. Prior studies suggest the importance of patient safety management [45] and awareness of patient safety culture [46] as predictive factors for patient safety activities in middle-sized hospitals. In this study, the experience of completing patient safety education within one year and awareness of patient engagement were found to be significantly associated with the performance of nursing services for patient engagement. Thus, it can be said that nurses should become aware of the importance of patient safety management and culture through relevant education, which can improve nursing performance for patient safety, including patient engagement.
This study's findings have confirmed the existence of a partial mediating effect of patient participation culture. Specifically, the result demonstrate that ethical leadership has a significant impact on performance in patient-engaged nursing services. This relationship is partially explained by the influence of patient participation culture. This means that the more positive the nursing staff recognizes the level of ethical leadership of nursing managers, the better the patient participation culture score, thus leading to an improvement of performance in patient-engaged nursing services. In other words, ethical leadership affects performance in patient-engaged nursing services through a patient participation culture, suggesting that the patient participation culture being recognized by nurses is crucial. In other words, in order for the ethical leadership of nursing managers to be expressed as the organizational outcome of performance in patient-engaged nursing services, the patient participation culture must be supported. These findings support the results of previous studies that ethical leadership affects nurses' service behaviors [47], perception of patient safety culture and organizational commitment [48], and patient safety activities like nursing error rates and error reporting [49]. Therefore, to promote patient safety performance, including patient engagement, it is necessary to seek ways to improve the ethical leadership of nursing unit managers and the patient participation culture of hospital organizations. Furthermore, the results of this study show that the score of performance in patient-engaged nursing services is high when patient safety education is completed and patient participation is recognized, suggesting that patient participation concepts and specific practice strategies should be provided through patient safety education.
The development of a solution is thus urgently needed for systemic elements, which are insufficiently performed nursing services that can facilitate patient engagement. Systemic elements include establishing a way for patients and their families to participate in decision-making, standardizing procedures for effective communication among medical staff, and enabling patients and families to express concerns to healthcare providers during discharge training. A systemic approach to patient safety has long been recognized for its effectiveness [50]. Therefore, the national policy should support establishing such a system, by suggesting guidelines to facilitate improvement at the organizational level and promoting patient engagement.
Several limitations of the study should be acknowledged. First the sample size is small. Moreover, the results have limited generalizability due to convenience sampling. Second, it is difficult to infer causality because of the cross-sectional design. Finally, ethical leadership, patient participation culture, and performance in patient-engaged nursing services were measured using self-reported questionnaires; thus, the results could be influenced by recall bias. Therefore, we recommend that objective indicators, such as patient satisfaction and patient safety accidents, be used to ensure objectivity in the provision of patient-engaged nursing services.
The results highlight the importance of ethical leadership and patient participation culture in increasing performance in patient-engaged nursing services, and it was empirically confirmed that patient participation culture has a partial mediating effect in the relationship between ethical leadership and performance in patient-engaged nursing services. To enhance patient engagement at the individual nurse's level, it is necessary to understand how to share health-related information and responsibility with patients and apply them skillfully in the treatment process, so that inexperienced nurses can improve their abilities. It also allows hospital managers to implement effective education strategies to enhance performance of patient-engaged nursing services by providing patient safety and patient engagement education.
To develop nursing competencies and reach a consensus on the effectiveness of patient engagement, nursing staff must be educated on patient engagement and safety. Furthermore, to promote patient-engaged nursing services, nurse managers' ethical leadership should be strengthened, and a patient participation culture should be developed at a policy level through systematic education on patient safety and engagement.
YeaSeul Yoon and Yoonjung Ji received a scholarship from Brain Korea 21 FOUR Project funded by the National Research Foundation of Korea.